

The clinical characteristics of dementia with Lewy bodies and a consideration of prodromal diagnosis
- PMID: 25484925
- PMCID: PMC4255387
- DOI: 10.1186/alzrt274
The clinical characteristics of dementia with Lewy bodies and a consideration of prodromal diagnosis
Abstract
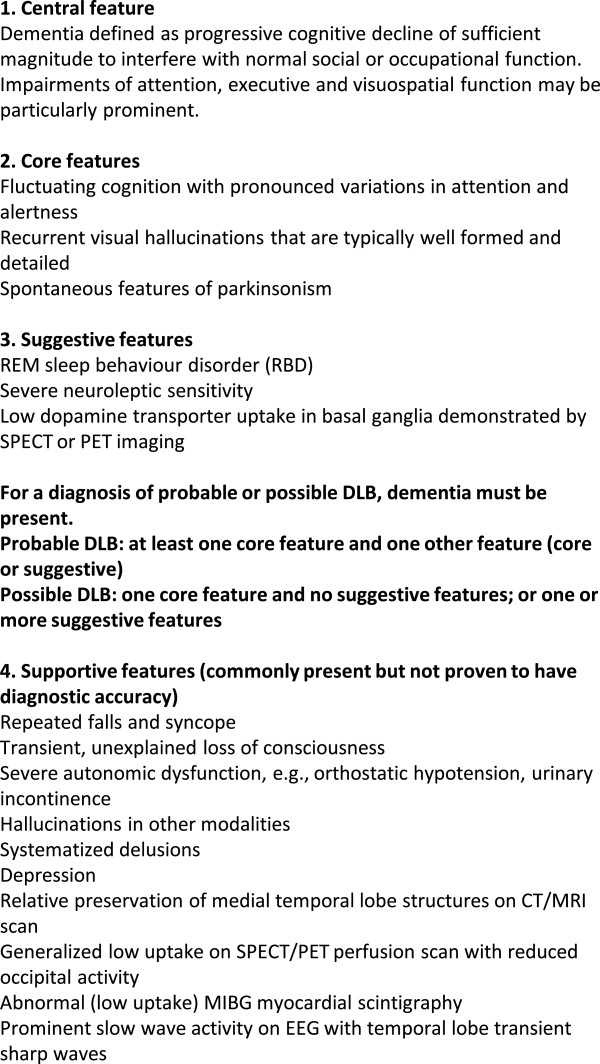
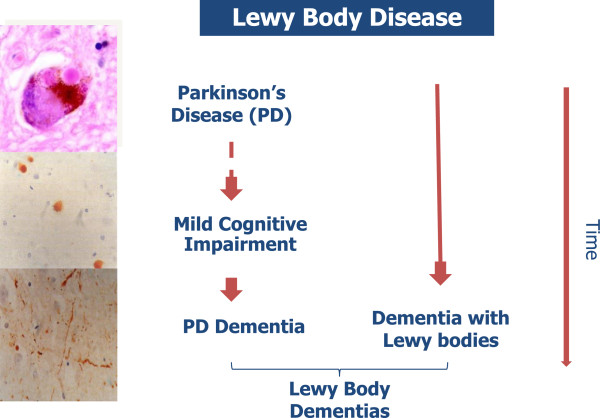
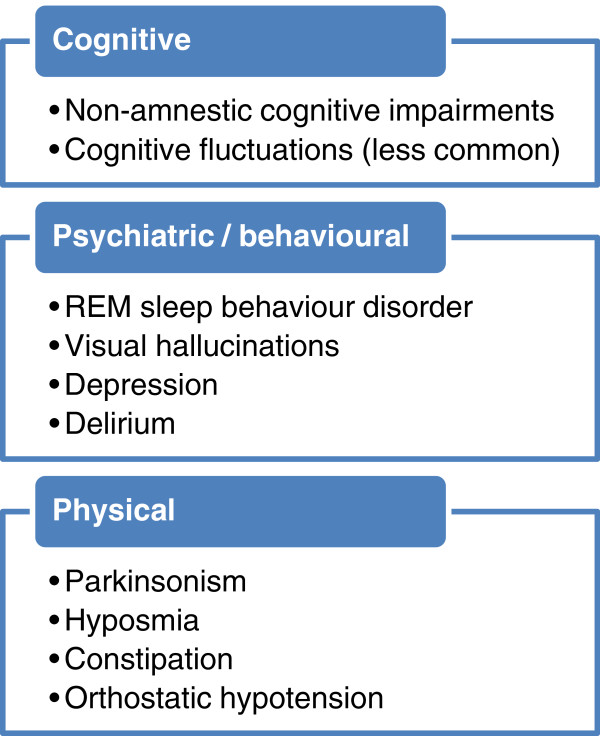
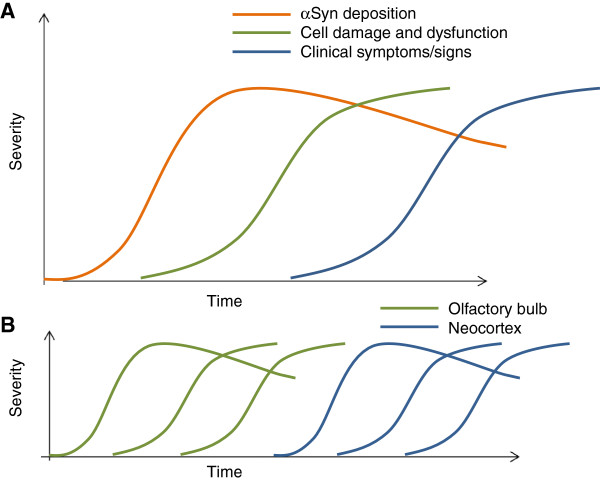
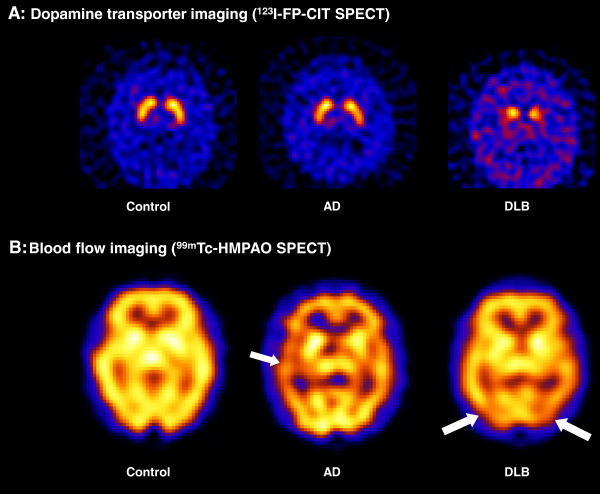
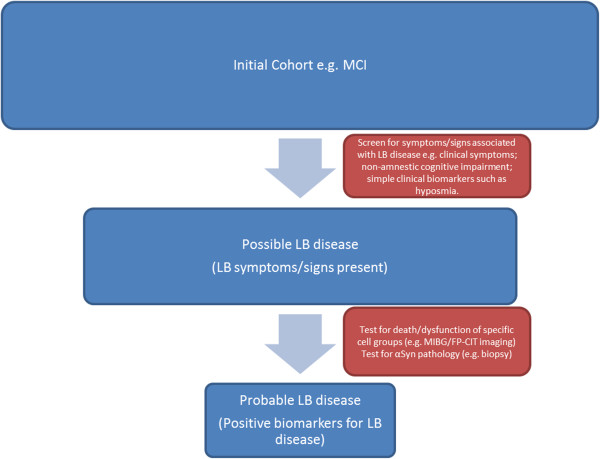
Dementia with Lewy bodies (DLB) is the second most common type of degenerative dementia following Alzheimer's disease (AD). DLB is clinically and pathologically related to Parkinson's disease (PD) and PD dementia, and the three disorders can be viewed as existing on a spectrum of Lewy body disease. In recent years there has been a concerted effort to establish the phenotypes of AD and PD in the prodromal phase (before the respective syndromes of cognitive and motor impairment are expressed). Evidence for the prodromal presentation of DLB is also emerging. This paper briefly reviews what is known about the clinical presentation of prodromal DLB before discussing the pathology of Lewy body disease and how this relates to potential biomarkers of prodromal DLB. The presenting features of DLB can be broadly placed in three categories: cognitive impairment (particularly nonamnestic cognitive impairments), behavioural/psychiatric phenomena (for example, hallucinations, rapid eye movement sleep behaviour disorder (RBD)) and physical symptoms (for example, parkinsonism, decreased sense of smell, autonomic dysfunction). Some noncognitive symptoms such as constipation, RBD, hyposmia and postural dizziness can predate the onset of memory impairment by several years in DLB. Pathological studies of Lewy body disease have found that the earliest sites of involvement are the olfactory bulb, the dorsal motor nucleus of the vagal nerve, the peripheral autonomic nervous system, including the enteric nervous system, and the brainstem. Some of the most promising early markers for DLB include the presence of RBD, autonomic dysfunction or hyposmia, (123)I-metaiodobenzylguanidine cardiac scintigraphy, measures of substantia nigra pathology and skin biopsy for α-synuclein in peripheral autonomic nerves. In the absence of disease-modifying therapies, the diagnosis of prodromal DLB is of limited use in the clinic. That said, knowledge of the prodromal development of DLB could help clinicians identify cases of DLB where the diagnosis is uncertain. Prodromal diagnosis is of great importance in research, where identifying Lewy body disease at an earlier stage may allow researchers to investigate the initial phases of dementia pathophysiology, develop treatments designed to interrupt the development of the dementia syndrome and accurately identify the patients most likely to benefit from these treatments.
Figures
References
-
- McKeith IG, Dickson DW, Lowe J, Emre M, O'Brien JT, Feldman H, Cummings J, Duda JE, Lippa C, Perry EK, Aarsland D, Arai H, Ballard CG, Boeve B, Burn DJ, Costa D, Del Ser T, Dubois B, Galasko D, Gauthier S, Goetz CG, Gomez-Tortosa E, Halliday G, Hansen LA, Hardy J, Iwatsubo T, Kalaria RN, Kaufer D, Kenny RA, Korczyn A. et al.Diagnosis and management of dementia with Lewy bodies. Neurology. 2005;65:1863–1872. doi: 10.1212/01.wnl.0000187889.17253.b1. - DOI - PubMed
-
- Emre M, Aarsland D, Brown R, Burn DJ, Duyckaerts C, Mizuno Y, Broe GA, Cummings J, Dickson DW, Gauthier S, Goldman J, Goetz C, Korczyn A, Lees A, Levy R, Litvan I, McKeith I, Olanow W, Poewe W, Quinn N, Sampaio C, Tolosa E, Dubois B. Clinical diagnostic criteria for dementia associated with Parkinson's disease. Mov Disord. 2007;22:1689–1707. doi: 10.1002/mds.21507. quiz 1837. - DOI - PubMed
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5. Arlington, VA: American Psychiatric Publishing; 2013.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
