

Robotically enhanced coronary artery bypass surgery
- PMID: 25484967
- PMCID: PMC4247435
- DOI: 10.1007/s11701-007-0029-7
Robotically enhanced coronary artery bypass surgery
Abstract
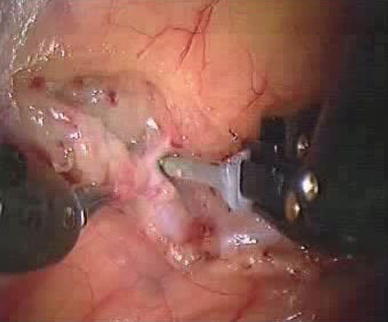
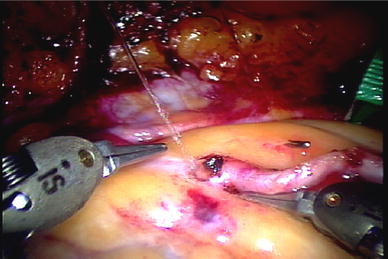
Robotically enhanced telemanipulation surgery is a rapidly developing technique which enables totally endoscopic cardiac surgery with utmost precision and perfection on both beating heart and arrested heart. Between December 2002 and September 2006, 268 patients underwent robotically enhanced coronary artery bypass surgery using the da Vinci telemanipulation system. Fourteen patients underwent total endoscopic coronary artery bypass surgery. Of these 12 were performed on a beating heart and 2 on an arrested heart. Two-hundred and fifty-four patients had endoscopic takedown of the internal mammary artery followed by minimally invasive direct coronary artery bypass in 193 patients and left anterolateral thoracotomy in 61 patients. The internal mammary artery mobilization time was 36 min (28-76 min) and the left internal mammary artery to left anterior descending artery anastomosis time ranged from 20 to 36 min for the totally endoscopic coronary artery bypass patients. The right internal mammary artery of one patient was anastomosed to diagonal artery totally endoscopically. The mean internal mammary artery flow by Doppler measurement in patients undergoing minimally invasive direct coronary artery bypass was 58 ml min(-1). Seven patients required conversion to median sternotomy and coronary bypass surgery on the beating heart. The mean intensive care unit stay was 1.2 days and the mean hospital stay 4.5 days. There was one in-hospital mortality. All 14 patients who underwent total endoscopic bypass surgery had coronary angiography 3 months later which showed 100% patency in 13 patients. One patient had 50% anastomotic narrowing for which coronary angioplasty was performed in the same sitting. By using telematic technology, a complete endoscopic anastomosis is possible in both single vessels and suitable double vessel disease patients. The use of robotics is now extended to achieve complete myocardial revascularization by harvesting both the internal mammary arteries and making a small thoracotomy for direct anastomosis also.
Keywords: Coronary artery bypass grafting; Coronary artery disease; Minimally invasive surgery.
Figures



Similar articles
-
Robotically enhanced coronary artery bypass surgery.Indian Heart J. 2004 Nov-Dec;56(6):622-7. Indian Heart J. 2004. PMID: 15751517
-
Totally endoscopic coronary artery bypass surgery.Asian Cardiovasc Thorac Ann. 2006 Dec;14(6):447-51. doi: 10.1177/021849230601400601. Asian Cardiovasc Thorac Ann. 2006. PMID: 17130316
-
Computer-enhanced "robotic" cardiac surgery: experience in 148 patients.J Thorac Cardiovasc Surg. 2001 May;121(5):842-53. doi: 10.1067/mtc.2001.112625. J Thorac Cardiovasc Surg. 2001. PMID: 11326227
-
Totally endoscopic coronary artery bypass grafting on the arrested heart.Heart Surg Forum. 2007;10(4):E338-43. doi: 10.1532/HSF98.20070710. Heart Surg Forum. 2007. PMID: 17650461 Review.
-
Robotic totally endoscopic multivessel coronary artery bypass grafting: procedure development, challenges, results.Innovations (Phila). 2012 Jan-Feb;7(1):3-8. doi: 10.1097/IMI.0b013e3182552ea8. Innovations (Phila). 2012. PMID: 22576029 Review.
Cited by
-
Comparing the Effectiveness of Open and Minimally Invasive Approaches in Coronary Artery Bypass Grafting: A Systematic Review.Clin Pract. 2024 Sep 10;14(5):1842-1868. doi: 10.3390/clinpract14050147. Clin Pract. 2024. PMID: 39311297 Free PMC article. Review.
-
Systematic review and meta-analysis of two decades of reported outcomes for robotic coronary artery bypass grafting.Ann Cardiothorac Surg. 2024 Jul 31;13(4):311-325. doi: 10.21037/acs-2023-rcabg-0191. Epub 2024 Jul 26. Ann Cardiothorac Surg. 2024. PMID: 39157187 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
