

American trends in expectant management utilization for prostate cancer from 2000 to 2009
- PMID: 25485003
- PMCID: PMC4250240
- DOI: 10.5489/cuaj.2073
American trends in expectant management utilization for prostate cancer from 2000 to 2009
Abstract
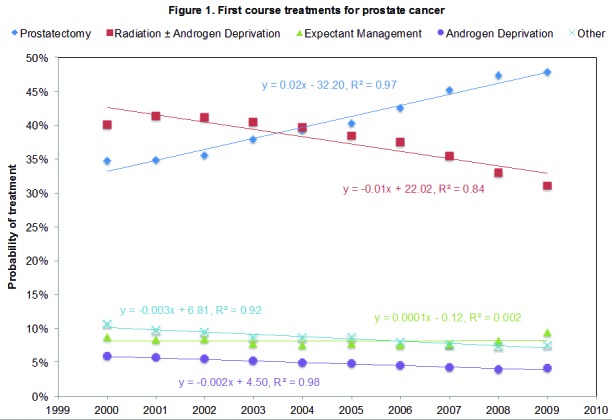
Introducton: The overtreatment of early prostate cancer has become a major public health concern. Expectant management (EM) is a strategy to minimize overtreatment, but little is known about its pattern of use. We sought to examine national EM utilization over the preceding decade.
Methods: We examined prostate cancer treatment utilization from 2000 to 2009 using the National Cancer Database. EM use was analyzed in relation to other treatments and by cancer stage, age group, Charlson score, and hospital practice setting.
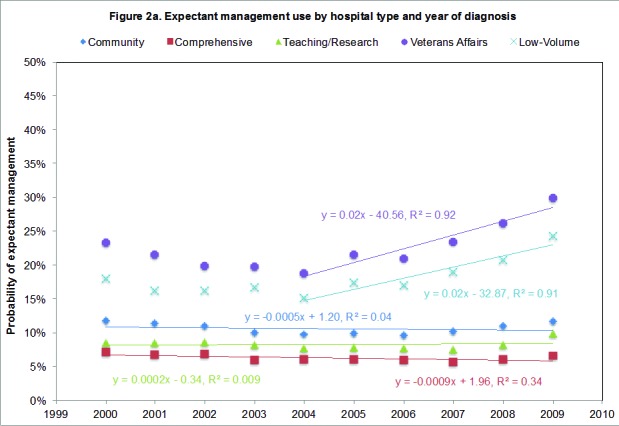
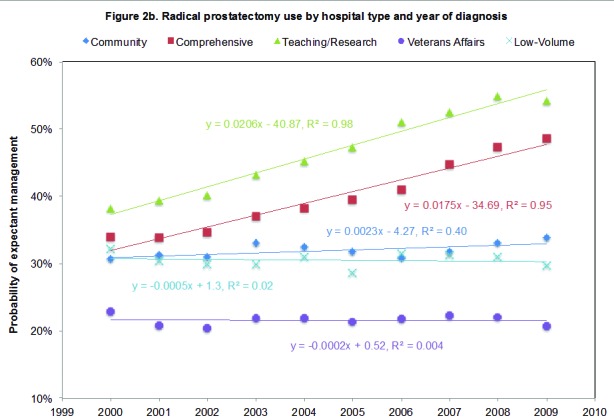
Results: Overall, 109 997 (8.2%) men were managed initially with EM. EM usage remained stable at 7.6% to 9.5% from 2000 to 2009 with no appreciable increase for low-stage cancers. Usage was only slightly higher in elderly patients and in patients with multiple comorbidities. Veterans Affairs and low-volume hospitals had a much higher and increasing EM rate (range: 18.8%-29.8% and 15.1%-24.2%, respectively), compared to community hospitals, comprehensive cancer centres, and teaching hospitals, which showed no increased adoption. On further analysis, EM use remained high for low-stage cancers at Veterans Affairs and low-volume hospitals (24.0% and 19.1%, respectively), regardless of age or comorbidity, a pattern not shared by other practice settings.
Conclusions: EM utilization remained low and stable last decade, regardless of disease or patient characteristics. Conversely, Veterans Affairs and low-volume hospitals led the trend in national EM adoption, particularly in men with low-stage cancers and limited life expectancies. The limitations of this dataset preclude any determination of the appropriateness of EM utilization. Nonetheless, further study is needed to identify factors influencing EM adoption to ensure its proper use in the future.
Figures
Similar articles
-
Utilization and predictors of expectant management among elderly men with low-and intermediate-risk localized prostate cancer in U.S. urological practice.Urol Pract. 2017 Mar;4(2):132-139. doi: 10.1016/j.urpr.2016.05.005. Urol Pract. 2017. PMID: 28808670 Free PMC article.
-
How older patients' treatment preferences are influenced by disclosures about therapeutic uncertainty: surgery versus expectant management for localized prostate cancer.J Am Geriatr Soc. 1996 Aug;44(8):934-7. doi: 10.1111/j.1532-5415.1996.tb01863.x. J Am Geriatr Soc. 1996. PMID: 8708303
-
Matching tumor risk with aggressiveness of treatment in men with multiple comorbidities and early-stage prostate cancer.Cancer. 2013 Oct 1;119(19):3446-53. doi: 10.1002/cncr.28226. Epub 2013 Jul 16. Cancer. 2013. PMID: 23861016
-
Expectant management of veterans with early-stage prostate cancer.Cancer. 2016 Feb 15;122(4):626-33. doi: 10.1002/cncr.29785. Epub 2015 Nov 5. Cancer. 2016. PMID: 26540451
-
An evidence review of active surveillance in men with localized prostate cancer.Evid Rep Technol Assess (Full Rep). 2011 Dec;(204):1-341. Evid Rep Technol Assess (Full Rep). 2011. PMID: 23126653 Free PMC article. Review.
Cited by
-
A hospital-based study of initial observation for low-risk prostate cancer and its predictors in the United States.Can Urol Assoc J. 2015 Mar-Apr;9(3-4):E193-9. doi: 10.5489/cuaj.2606. Epub 2015 Apr 13. Can Urol Assoc J. 2015. PMID: 26770290 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
