

Acute and perioperative care of the burn-injured patient
- PMID: 25485468
- PMCID: PMC4844008
- DOI: 10.1097/ALN.0000000000000559
Acute and perioperative care of the burn-injured patient
Abstract
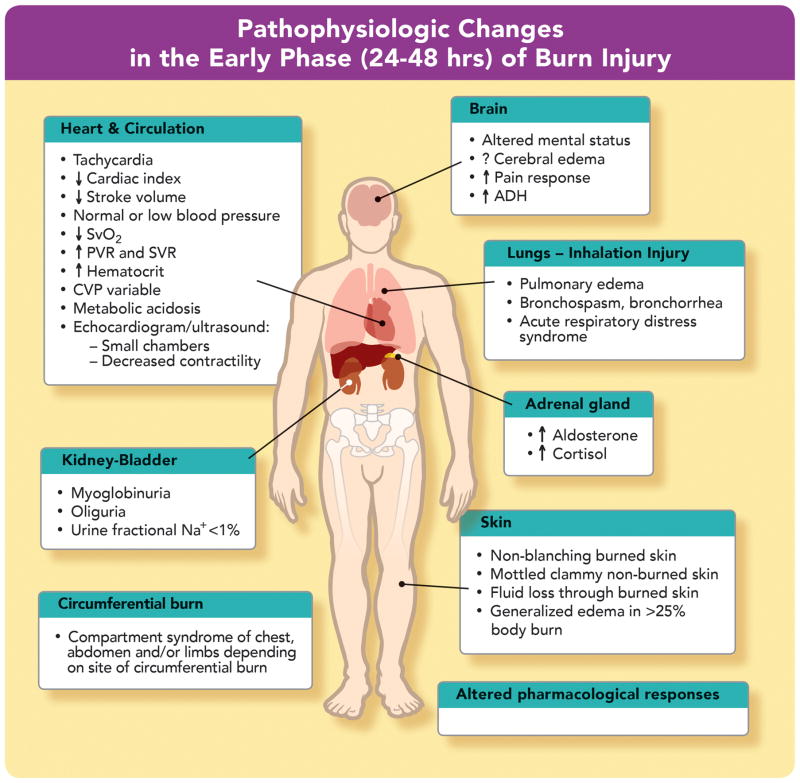
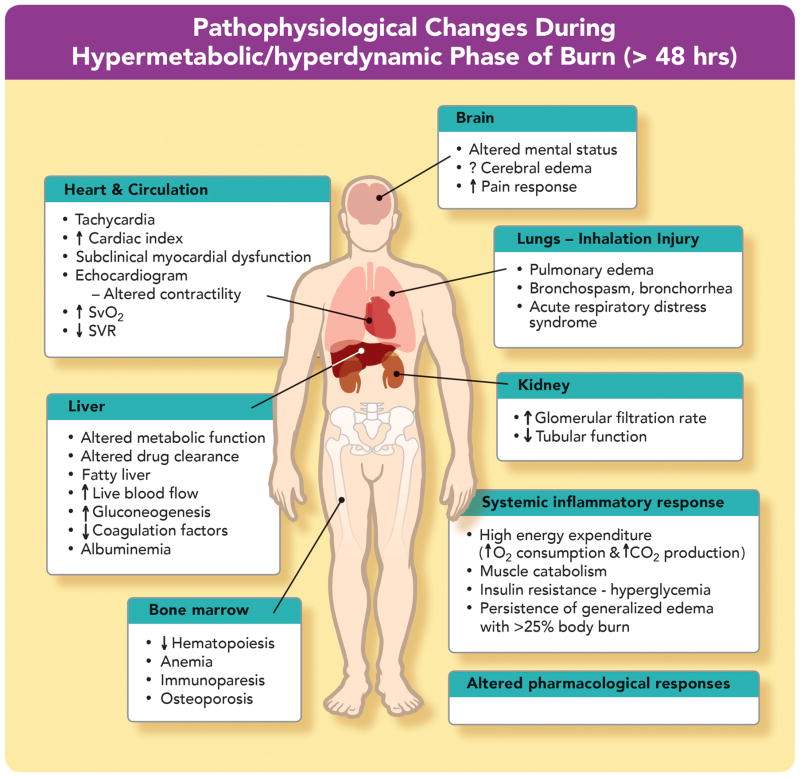
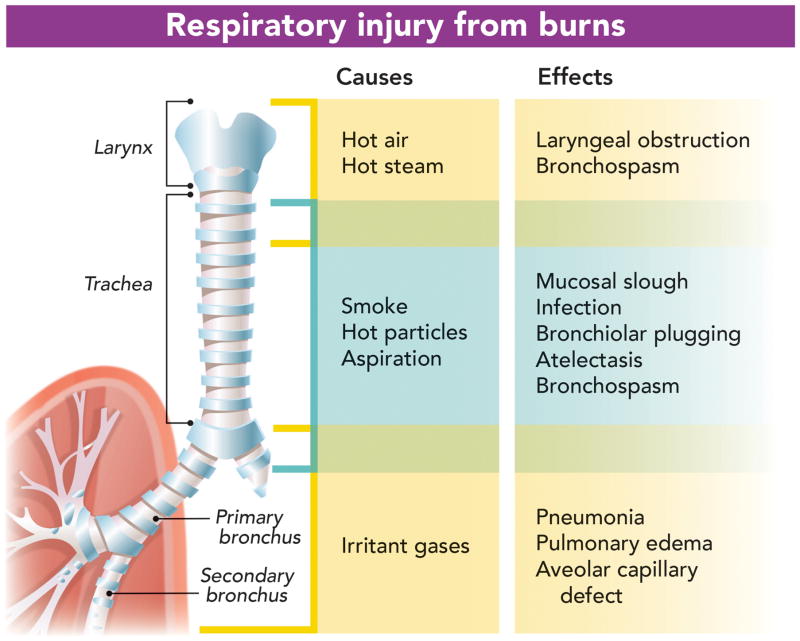
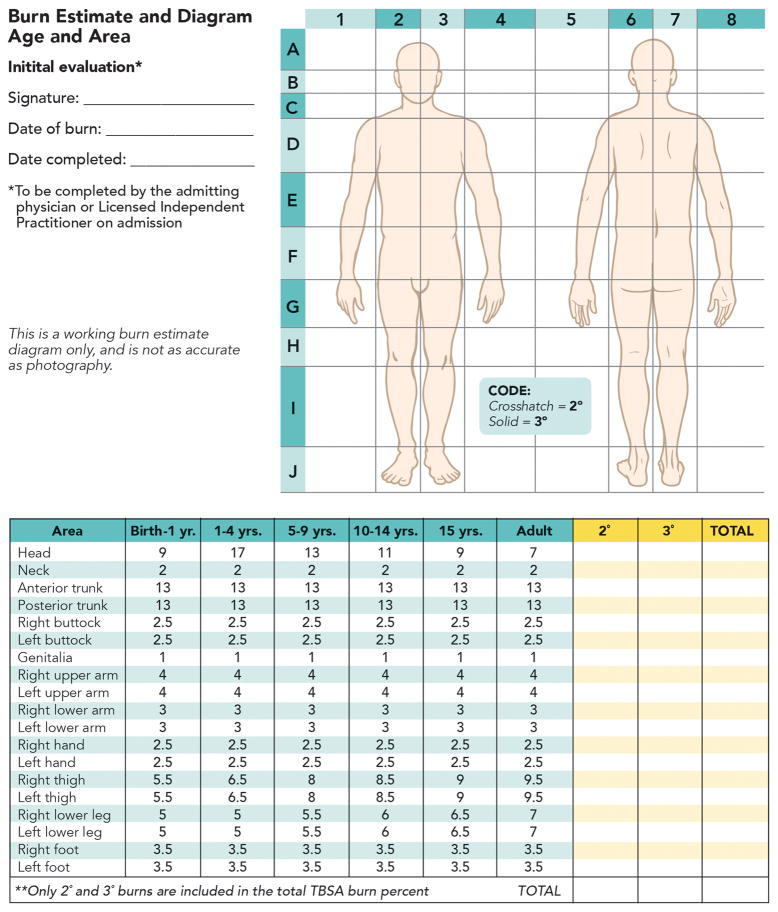
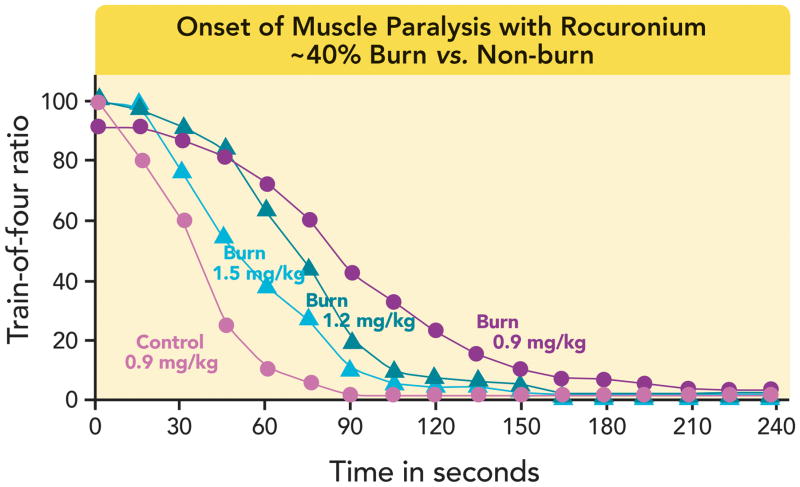
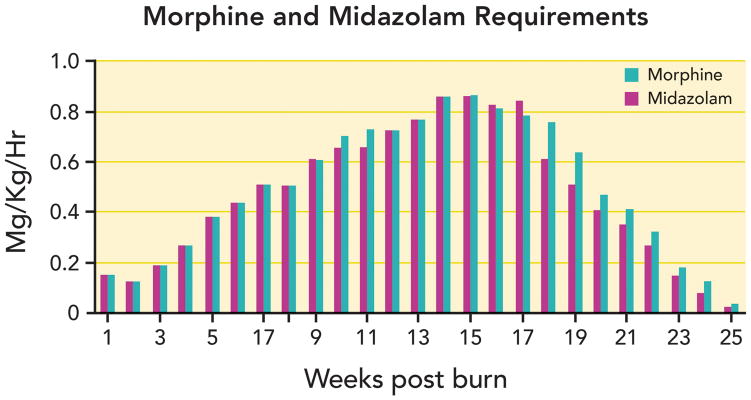
Care of burn-injured patients requires knowledge of the pathophysiologic changes affecting virtually all organs from the onset of injury until wounds are healed. Massive airway and/or lung edema can occur rapidly and unpredictably after burn and/or inhalation injury. Hemodynamics in the early phase of severe burn injury is characterized by a reduction in cardiac output and increased systemic and pulmonary vascular resistance. Approximately 2 to 5 days after major burn injury, a hyperdynamic and hypermetabolic state develops. Electrical burns result in morbidity much higher than expected based on burn size alone. Formulae for fluid resuscitation should serve only as guideline; fluids should be titrated to physiologic endpoints. Burn injury is associated basal and procedural pain requiring higher than normal opioid and sedative doses. Operating room concerns for the burn-injured patient include airway abnormalities, impaired lung function, vascular access, deceptively large and rapid blood loss, hypothermia, and altered pharmacology.
Conflict of interest statement
The authors declare no competing interests
Figures

References
-
- Cuthbertson DP. Postshock metabolic response. Lancet. 1942;239:433–7.
-
- Martyn JA, Aikawa N, Wilson RS, Szyfelbein SK, Burke JF. Extrapulmonary factors influencing the ration of arterial oxygen tension to inspired oxygen concentration in burn patients. Crit Care Med. 1979;7:492–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
