

Descriptive epidemiology of typhoid fever during an epidemic in Harare, Zimbabwe, 2012
- PMID: 25486292
- PMCID: PMC4259398
- DOI: 10.1371/journal.pone.0114702
Descriptive epidemiology of typhoid fever during an epidemic in Harare, Zimbabwe, 2012
Abstract
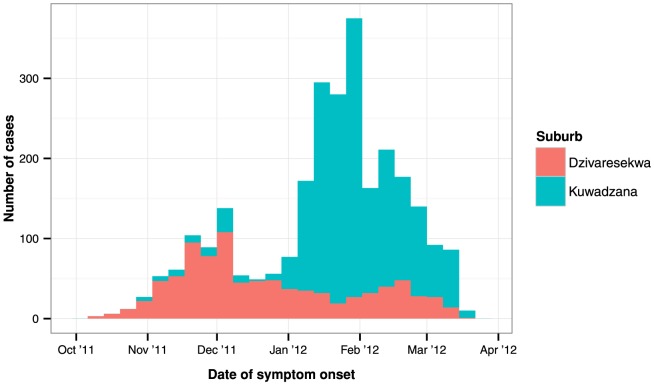
Background: Typhoid fever remains a significant public health problem in developing countries. In October 2011, a typhoid fever epidemic was declared in Harare, Zimbabwe - the fourth enteric infection epidemic since 2008. To orient control activities, we described the epidemiology and spatiotemporal clustering of the epidemic in Dzivaresekwa and Kuwadzana, the two most affected suburbs of Harare.
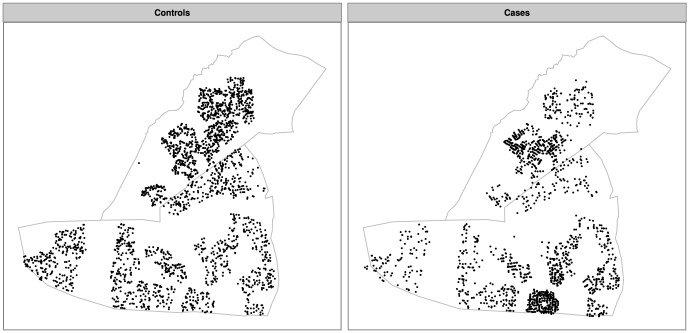
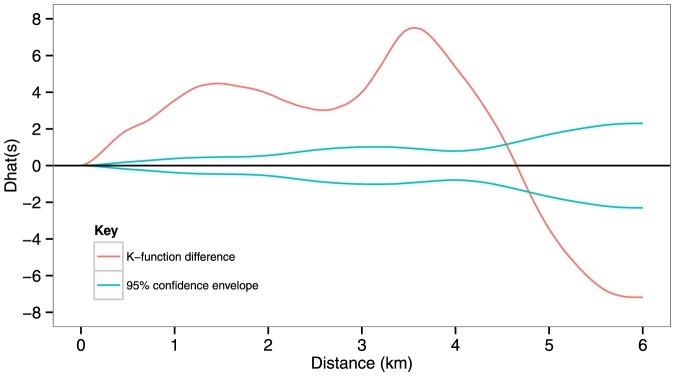
Methods: A typhoid fever case-patient register was analysed to describe the epidemic. To explore clustering, we constructed a dataset comprising GPS coordinates of case-patient residences and randomly sampled residential locations (spatial controls). The scale and significance of clustering was explored with Ripley K functions. Cluster locations were determined by a random labelling technique and confirmed using Kulldorff's spatial scan statistic.
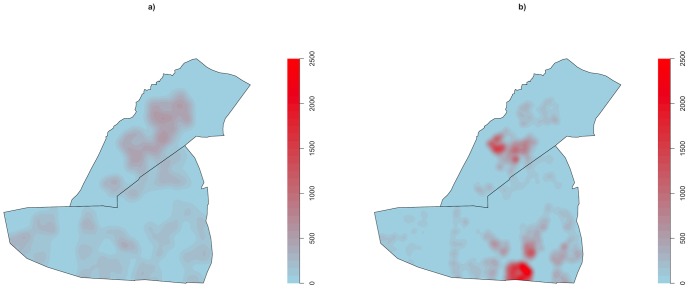
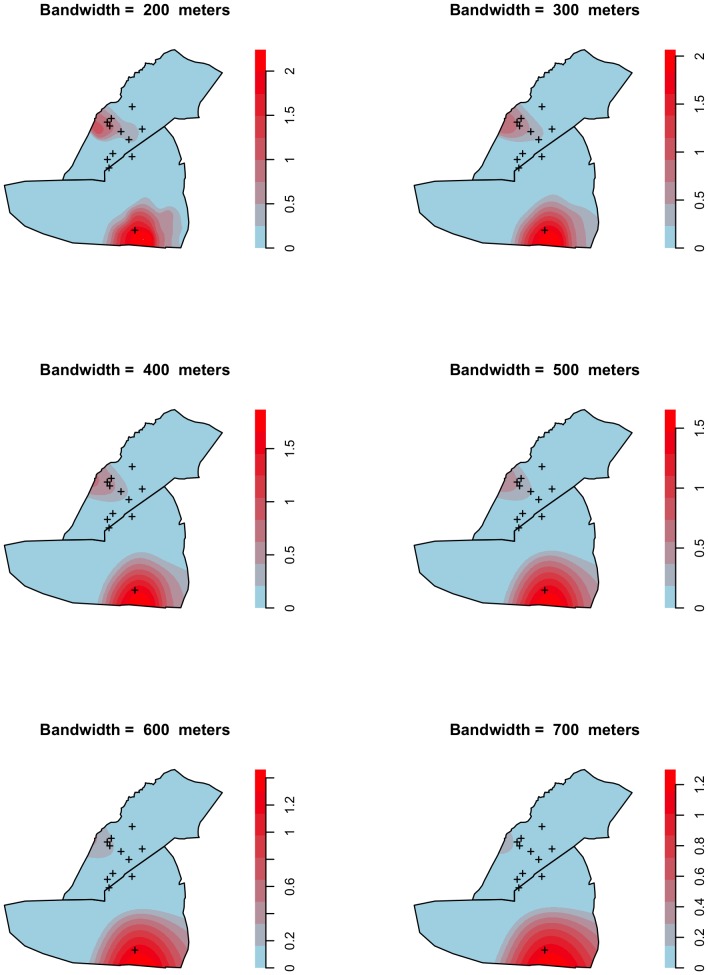
Principal findings: We analysed data from 2570 confirmed and suspected case-patients, and found significant spatiotemporal clustering of typhoid fever in two non-overlapping areas, which appeared to be linked to environmental sources. Peak relative risk was more than six times greater than in areas lying outside the cluster ranges. Clusters were identified in similar geographical ranges by both random labelling and Kulldorff's spatial scan statistic. The spatial scale at which typhoid fever clustered was highly localised, with significant clustering at distances up to 4.5 km and peak levels at approximately 3.5 km. The epicentre of infection transmission shifted from one cluster to the other during the course of the epidemic.
Conclusions: This study demonstrated highly localised clustering of typhoid fever during an epidemic in an urban African setting, and highlights the importance of spatiotemporal analysis for making timely decisions about targetting prevention and control activities and reinforcing treatment during epidemics. This approach should be integrated into existing surveillance systems to facilitate early detection of epidemics and identify their spatial range.
Conflict of interest statement
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
