

The epidemiological impact of HIV antiretroviral therapy on malaria in children
- PMID: 25486414
- PMCID: PMC4391884
- DOI: 10.1097/QAD.0000000000000550
The epidemiological impact of HIV antiretroviral therapy on malaria in children
Abstract
Objective: The objective of this study is to determine the epidemiological effectiveness of a first-line antiretroviral regimen with HIV protease inhibitor for preventing recurrent malaria in children under the range of HIV prevalence levels and malaria transmission intensities encountered in sub-Saharan Africa.
Design: A dynamic model of malaria transmission was developed using clinical data on the protease inhibitor extended posttreatment prophylactic effect of the antimalarial treatment, artemether-lumefantrine, in addition to parameter estimates from the literature.
Methods: To evaluate the benefits of HIV protease inhibitors on the health burden of recurrent malaria among children, we constructed a dynamic model of malaria transmission to both HIV-positive and HIV-negative children, parameterized by data from a recent clinical trial. The model was then evaluated under varying malaria transmission and HIV prevalence settings to determine the health benefits of HIV protease inhibitors in the context of artemether-lumefantrine treatment of malaria in children.
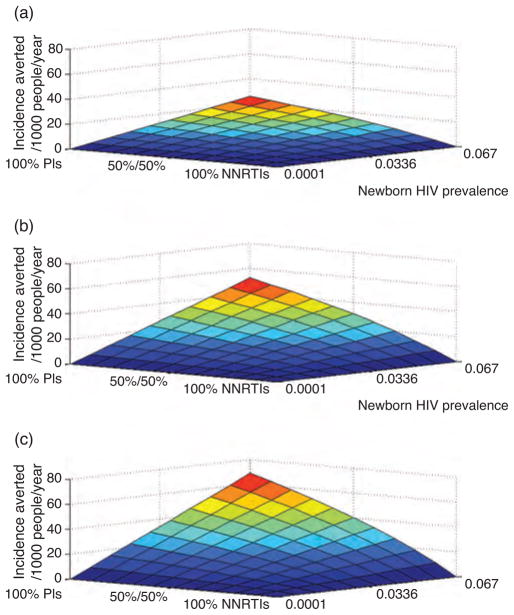
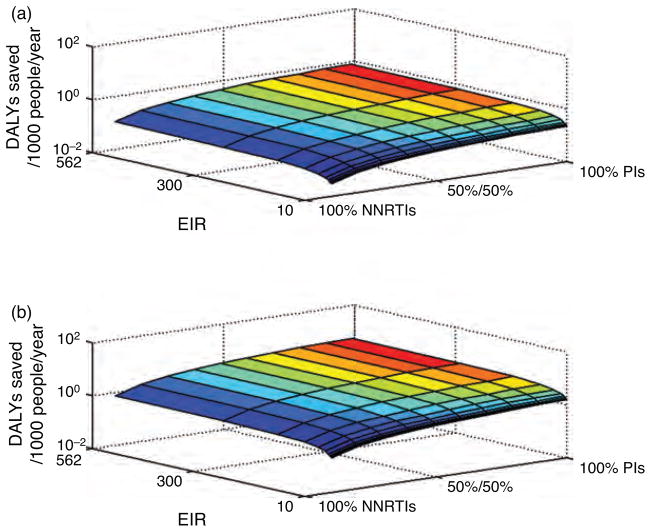
Results: Comparing scenarios of low, intermediate and high newborn HIV prevalence, in a range of malaria transmission settings, our dynamic model predicts that artemether-lumefantrine with HIV protease inhibitor based regimens prevents 0.03-0.10, 5.2-13.0 and 25.5-65.8 annual incidences of malaria per 1000 children, respectively. In addition, HIV protease inhibitors save 0.002-0.006, 0.22-0.8, 1.04-4.3 disability-adjusted life-years per 1000 children annually. Considering only HIV-infected children, HIV protease inhibitors avert between 278 and 1043 annual incidences of malaria per 1000 children.
Conclusion: The use of HIV protease inhibitor based regimens as first-line antiretroviral therapy for HIV is an effective measure for reducing recurrent malaria among HIV-infected children in areas where HIV and malaria are coendemic, and artemether-lumefantrine is a first-line antimalarial.
Conflict of interest statement
The authors do not have either a commercial or other association that might pose a conflict of interest.
Figures
References
-
- Flateau C, Le Loup G, Pialoux G. Consequences of HIV infection on malaria and therapeutic implications: a systematic review. Lancet Infect Dis. 2011;11:541–556. - PubMed
-
- WHO. Consolidated ARV guidelines 2013. Geneva: WHO; 2013.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
