

Benefits, harms, and cost-effectiveness of supplemental ultrasonography screening for women with dense breasts
- PMID: 25486550
- PMCID: PMC4314343
- DOI: 10.7326/M14-0692
Benefits, harms, and cost-effectiveness of supplemental ultrasonography screening for women with dense breasts
Abstract
Background: Many states have laws requiring mammography facilities to tell women with dense breasts and negative results on screening mammography to discuss supplemental screening tests with their providers. The most readily available supplemental screening method is ultrasonography, but little is known about its effectiveness.
Objective: To evaluate the benefits, harms, and cost-effectiveness of supplemental ultrasonography screening for women with dense breasts.
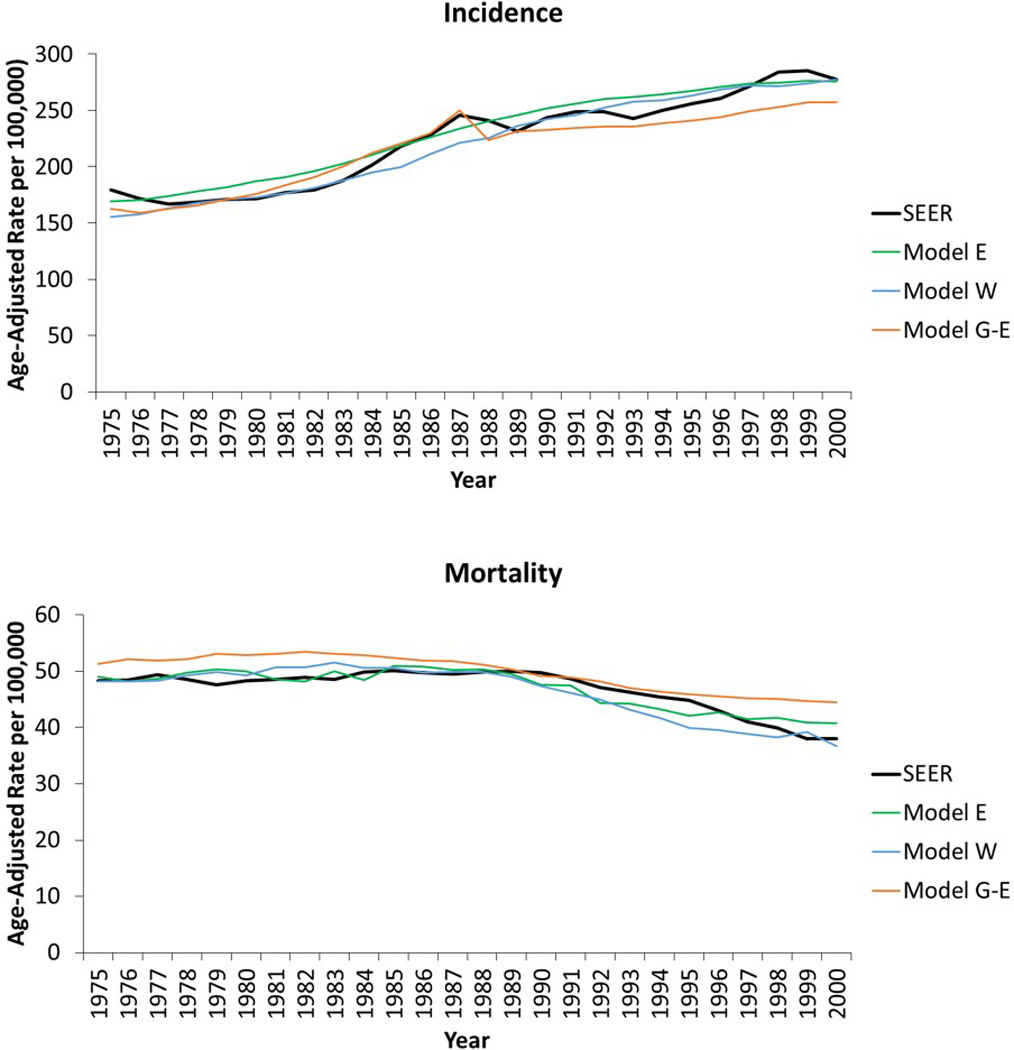
Design: Comparative modeling with 3 validated simulation models.
Data sources: Surveillance, Epidemiology, and End Results Program; Breast Cancer Surveillance Consortium; and medical literature.
Target population: Contemporary cohort of women eligible for routine screening.
Time horizon: Lifetime.
Perspective: Payer.
Intervention: Supplemental ultrasonography screening for women with dense breasts after a negative screening mammography result.
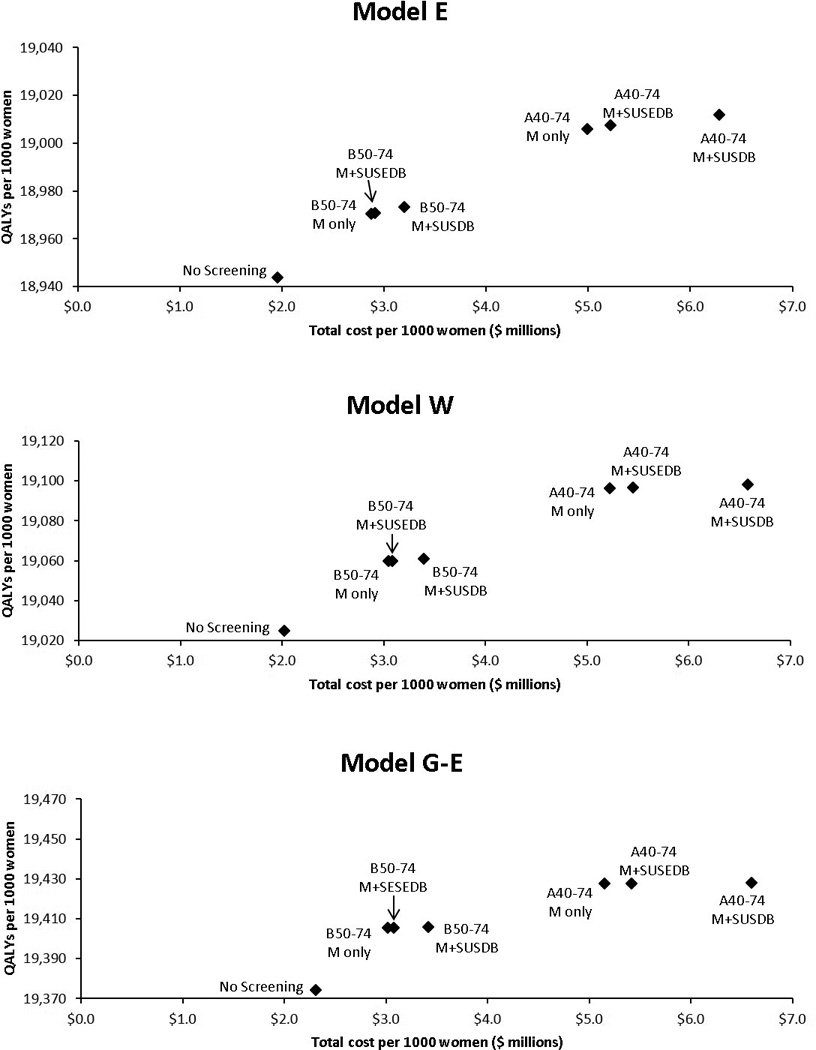
Outcome measures: Breast cancer deaths averted, quality-adjusted life-years (QALYs) gained, biopsies recommended after a false-positive ultrasonography result, and costs.
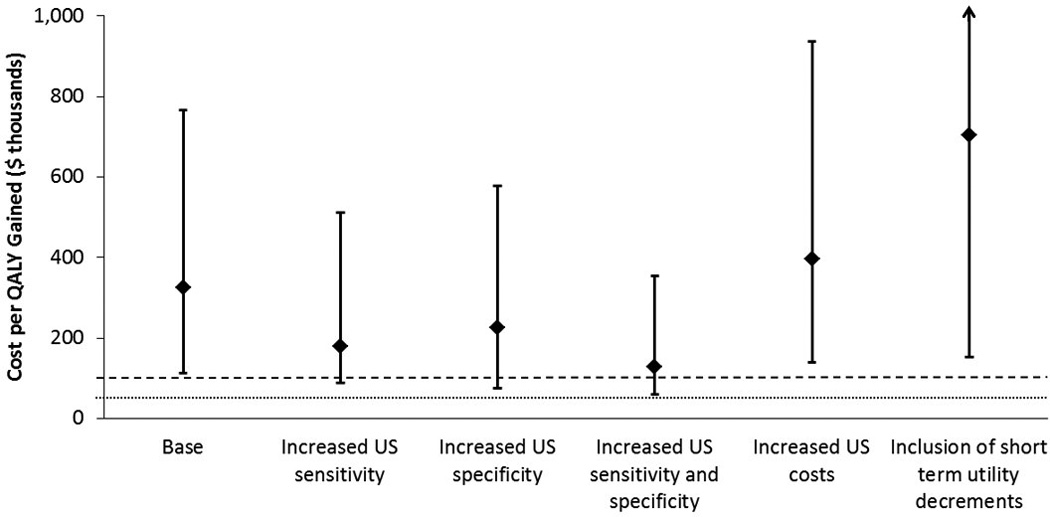
Results of base-case analysis: Supplemental ultrasonography screening after a negative mammography result for women aged 50 to 74 years with heterogeneously or extremely dense breasts averted 0.36 additional breast cancer deaths (range across models, 0.14 to 0.75), gained 1.7 QALYs (range, 0.9 to 4.7), and resulted in 354 biopsy recommendations after a false-positive ultrasonography result (range, 345 to 421) per 1000 women with dense breasts compared with biennial screening by mammography alone. The cost-effectiveness ratio was $325,000 per QALY gained (range, $112,000 to $766,000). Supplemental ultrasonography screening for only women with extremely dense breasts cost $246,000 per QALY gained (range, $74,000 to $535,000).
Results of sensitivity analysis: The conclusions were not sensitive to ultrasonography performance characteristics, screening frequency, or starting age.
Limitation: Provider costs for coordinating supplemental ultrasonography were not considered.
Conclusion: Supplemental ultrasonography screening for women with dense breasts would substantially increase costs while producing relatively small benefits.
Primary funding source: National Cancer Institute.
Figures
Comment in
-
Supplemental ultrasonography screening for women with dense breasts.Ann Intern Med. 2015 Jun 2;162(11):801. doi: 10.7326/L15-5061. Ann Intern Med. 2015. PMID: 26030640 No abstract available.
-
Supplemental ultrasonography screening for women with dense breasts.Ann Intern Med. 2015 Jun 2;162(11):801-2. doi: 10.7326/L15-5061-2. Ann Intern Med. 2015. PMID: 26030641 No abstract available.
-
Supplemental ultrasonography screening for women with dense breasts.Ann Intern Med. 2015 Jun 2;162(11):802. doi: 10.7326/L15-5061-3. Ann Intern Med. 2015. PMID: 26030642 No abstract available.
-
Supplemental ultrasonography screening for women with dense breasts.Ann Intern Med. 2015 Jun 2;162(11):802-3. doi: 10.7326/L15-5061-4. Ann Intern Med. 2015. PMID: 26030643 No abstract available.
References
-
- Boyd NF, Guo H, Martin LJ, Sun L, Stone J, Fishell E, et al. Mammographic density and the risk and detection of breast cancer. N Engl J Med. 2007;356(3):227–236. - PubMed
-
- Kerlikowske K, Grady D, Barclay J, Sickles EA, Ernster V. Effect of age, breast density, and family history on the sensitivity of first screening mammography. JAMA. 1996;276(1):33–38. - PubMed
-
- Buist DS, Porter PL, Lehman C, Taplin SH, White E. Factors contributing to mammography failure in women aged 40–49 years. Journal of the National Cancer Institute. 2004;96(19):1432–1440. - PubMed
-
- Carney PA, Miglioretti DL, Yankaskas BC, Kerlikowske K, Rosenberg R, Rutter CM, et al. Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography. Ann Intern Med. 2003;138(3):168–175. - PubMed