

Neurally adjusted ventilatory assist
- PMID: 25486574
- PMCID: PMC4727498
- DOI: 10.1097/MCC.0000000000000167
Neurally adjusted ventilatory assist
Abstract
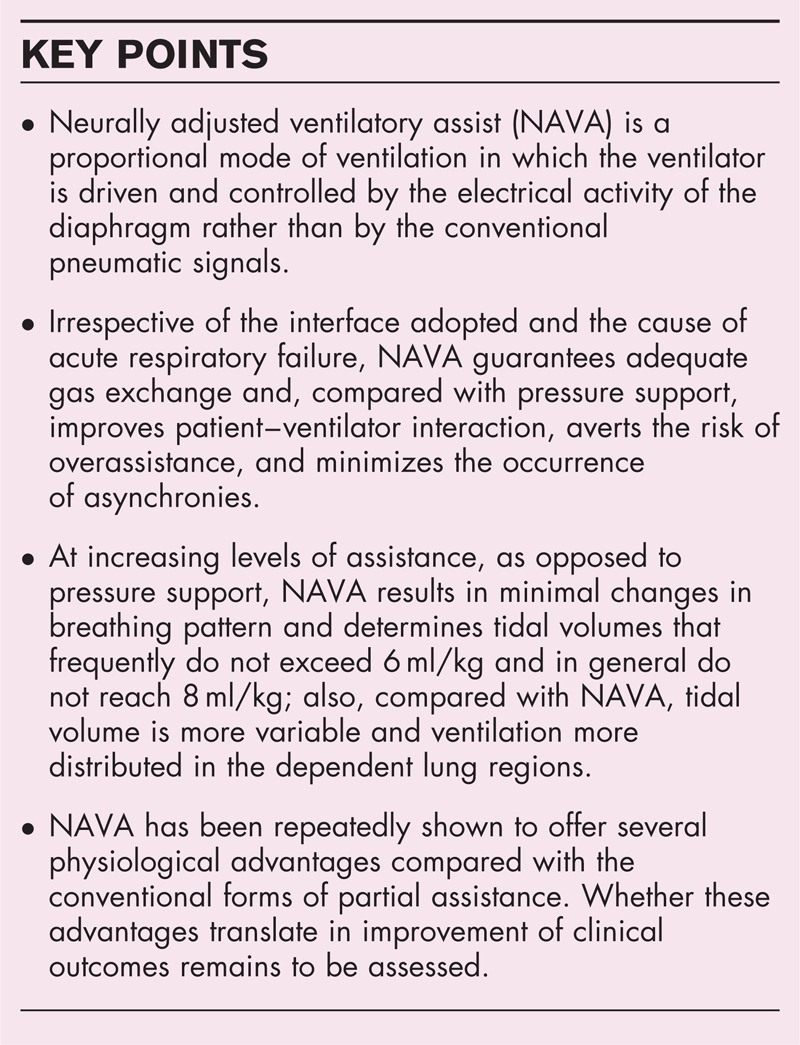
Purpose of review: Compared with the conventional forms of partial support, neurally adjusted ventilatory assist was repeatedly shown to improve patient-ventilator synchrony and reduce the risk of overassistance, while guaranteeing adequate inspiratory effort and gas exchange. A few animal studies also suggested the potential of neurally adjusted ventilatory assist in averting the risk of ventilator-induced lung injury. Recent work adds new information on the physiological effects of neurally adjusted ventilatory assist.
Recent findings: Compared with pressure support, neurally adjusted ventilatory assist has been shown to improve patient-ventilator interaction and synchrony in patients with the most challenging respiratory system mechanics, such as very low compliance consequent to severe acute respiratory distress syndrome and high resistance and air trapping due to chronic airflow obstruction; enhance redistribution of the ventilation in the dependent lung regions; avert the risk of patient-ventilator asynchrony due to sedation; avoid central apneas; limit the risk of high (injurious) tidal volumes in patients with acute respiratory distress syndrome of varied severity; and improve patient-ventilator interaction and synchrony during noninvasive ventilation, irrespective of the interface utilized.
Summary: Several studies nowadays prove the physiological benefits of neurally adjusted ventilatory assist, as opposed to the conventional modes of partial support. Whether these advantages translate into improvement of clinical outcomes remains to be determined.
Figures
References
-
- Sinderby C, Navalesi P, Beck J, et al. Neural control of mechanical ventilation in respiratory failure. Nat Med 1999; 5:1433–1436. - PubMed
-
- Navalesi P, Costa R. New modes of mechanical ventilation: proportional assist ventilation, neurally adjusted ventilatory assist, and fractal ventilation. Curr Opin Crit Care 2003; 9:51–58. - PubMed
-
- Bellani G, Mauri T, Coppadoro A, et al. Estimation of patient's inspiratory effort from the electrical activity of the diaphragm. Crit Care Med 2013; 41:1483–1491. - PubMed
-
- Colombo D, Cammarota G, Bergamaschi V, et al. Physiologic response to varying levels of pressure support and neurally adjusted ventilatory assist in patients with acute respiratory failure. Intensive Care Med 2008; 34:2010–2018. - PubMed
-
- Vaschetto R, Cammarota G, Colombo D, et al. Effects of propofol on patient–ventilator synchrony and interaction during pressure support ventilation and neurally adjusted ventilatory assist. Crit Care Med 2014; 42:74–82. - PubMed
-
In patients receiving partial ventilatory assistance for ARF of varied causes, propofol affects gas exchange and breathing pattern to an extent that varies with the depth of sedation and the mode of ventilation. EAdi is decreased at increasing levels of sedation with both pressure support and NAVA, although to varying extent. Deep propofol sedation deteriorates patient–ventilator interaction and may cause asynchrony during pressure support, but not in NAVA.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
