

Severe vivax malaria: a systematic review and meta-analysis of clinical studies since 1900
- PMID: 25486908
- PMCID: PMC4364574
- DOI: 10.1186/1475-2875-13-481
Severe vivax malaria: a systematic review and meta-analysis of clinical studies since 1900
Abstract
Background: Malaria caused by Plasmodium vivax was long considered to have a low mortality, but recent reports from some geographical areas suggest that severe and complicated vivax malaria may be more common than previously thought.
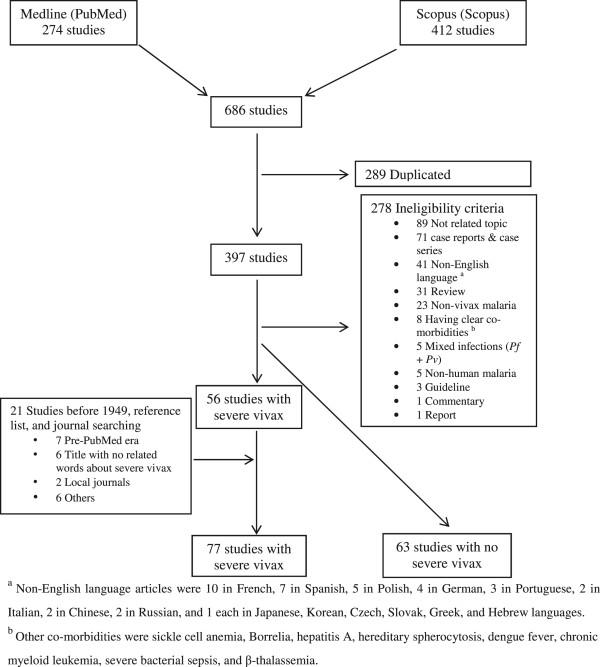
Methods: The primary objective of this systematic review and meta-analysis was to describe the reported clinical characteristics and the geographical variation in prevalence of reported severe vivax malaria and its change over time derived from English-language articles published since 1900. Medline and Scopus databases were searched for original papers on severe vivax malaria, using as inclusion criteria modified 2010 WHO criteria for the diagnosis of severe falciparum malaria. Articles before 1949 were identified through reference lists in journals, textbooks, and personal collections of colleagues.
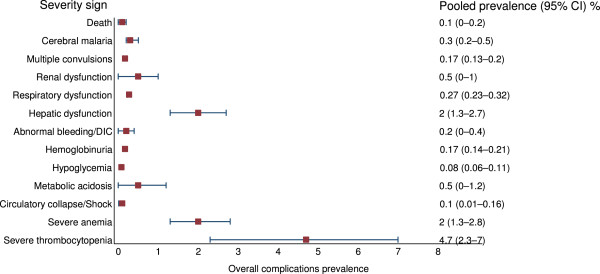
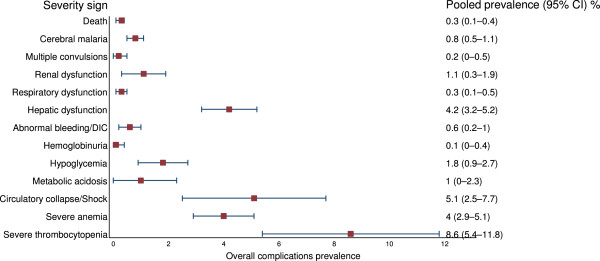
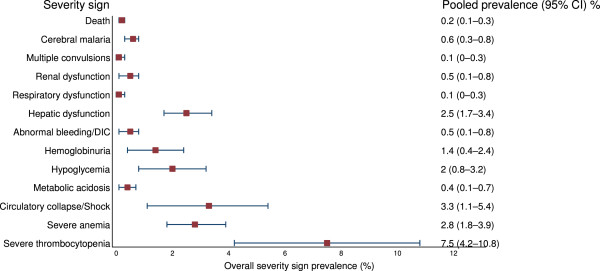
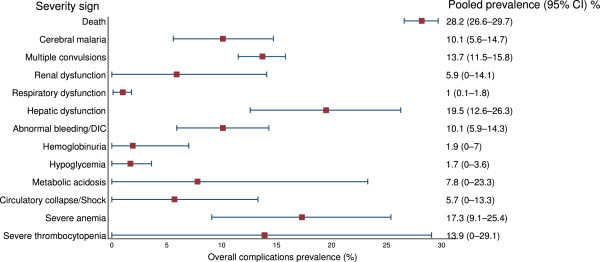
Results: A total of 77 studies with reported severe vivax malaria and 63 studies with no reported severe vivax malaria (totaling 46,411 and 6,753 vivax malaria patients, respectively) were included. The 77 studies with reported severe vivax malaria were mainly from India (n = 33), USA (n = 8), Indonesia (n = 6), and Pakistan (n = 6). Vivax endemic countries not reporting severe vivax malaria beyond individual case reports included: the Greater Mekong Sub-region, China, North Korea, Bangladesh, Afghanistan, Middle East (except Qatar), the horn of Africa, and Madagascar. Only 17/77 reports were from before 2000. Vivax mono-infection was confirmed by PCR in 14 studies and co-morbidities were ruled out in 23 studies. Among the 77 studies reporting severe vivax malaria, severe thrombocytopenia (<50,000/mm3) was the most common "severe" manifestation (888/45,775 with pooled prevalence of 8.6%). The case fatality was 0.3% (353/46,411). Severity syndromes varied widely between different geographical areas, with severe anaemia being most prominent in areas of high transmission and chloroquine resistance.
Conclusion: Plasmodium vivax can cause severe and even fatal disease, but there is a recent increase in reports over the past 15 years with larger series restricted to a limited number of geographical areas. The biological basis of these variations is currently not known. More detailed epidemiological studies are needed which dissociate causation from association to refine the definition and estimate the prevalence of severe vivax malaria.
Figures
References
-
- Guerra CA, Howes RE, Patil AP, Gething PW, Van Boeckel TP, Temperley WH, Kabaria CW, Tatem AJ, Manh BH, Elyazar IR, Baird JK, Snow RW, Hay SI. The international limits and population at risk of Plasmodium vivax transmission in 2009. PLoS Negl Trop Dis. 2010;4:e774. doi: 10.1371/journal.pntd.0000774. - DOI - PMC - PubMed
-
- Gething PW, Elyazar IRF, Moyes CL, Smith DL, Battle KE, Guerra CA, Patil AP, Tatem AJ, Howes RE, Myers MF, George DB, Horby P, Wertheim HF, Price RN, Jueller I, Baird JK, Hay SI. A long neglected world malaria map: Plasmodium vivax endemicity in 2010. PLoS Negl Trop Dis. 2012;6:e1814. doi: 10.1371/journal.pntd.0001814. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
