

Effect of human papillomavirus (HPV) vaccination on clinical indicators of sexual behaviour among adolescent girls: the Ontario Grade 8 HPV Vaccine Cohort Study
- PMID: 25487660
- PMCID: PMC4312170
- DOI: 10.1503/cmaj.140900
Effect of human papillomavirus (HPV) vaccination on clinical indicators of sexual behaviour among adolescent girls: the Ontario Grade 8 HPV Vaccine Cohort Study
Abstract
Background: Suboptimal human papillomavirus (HPV) vaccine coverage in some jurisdictions is partly attributed to fears that vaccination may increase risky sexual behaviour. We assessed the effect of HPV vaccination on clinical indicators of sexual behaviour among adolescent girls in Ontario.
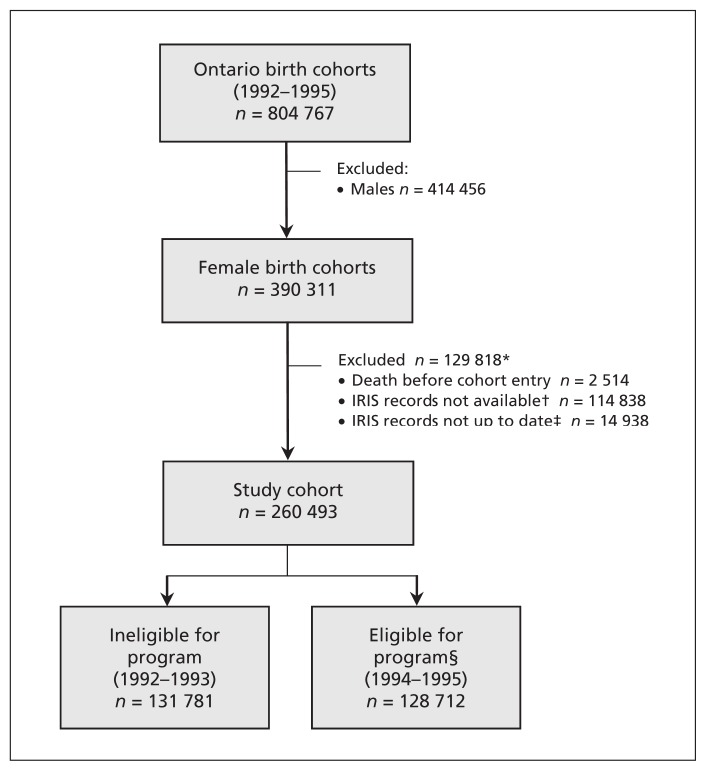
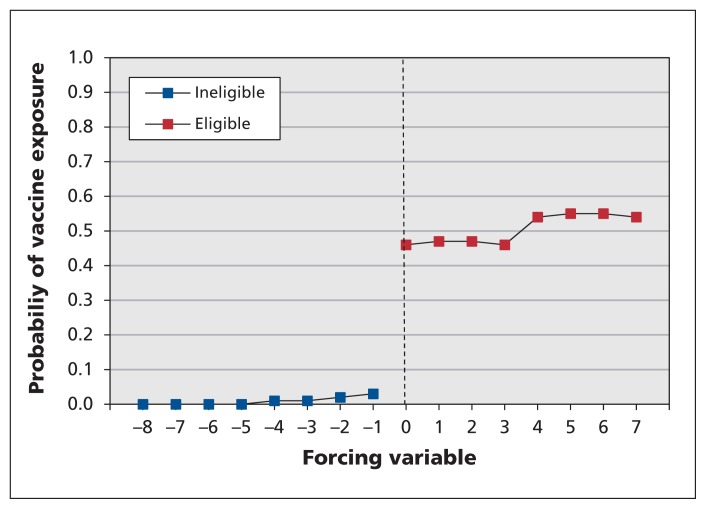
Methods: Using Ontario's administrative health databases, we identified a population-based cohort of girls in grade 8 in the 2 years before (2005/06 and 2006/07) and after (2007/08 and 2008/09) implementation of Ontario's grade 8 HPV vaccination program. For each girl, we then obtained data on vaccine receipt in grades 8 and 9 and data on indicators of sexual behaviour (pregnancy and non-HPV-related sexually transmitted infections) in grades 10-12. Using a quasi-experimental method known as regression discontinuity, we estimated, for each outcome, the risk difference (RD) and relative risk (RR) attributable to vaccination and to program eligibility.
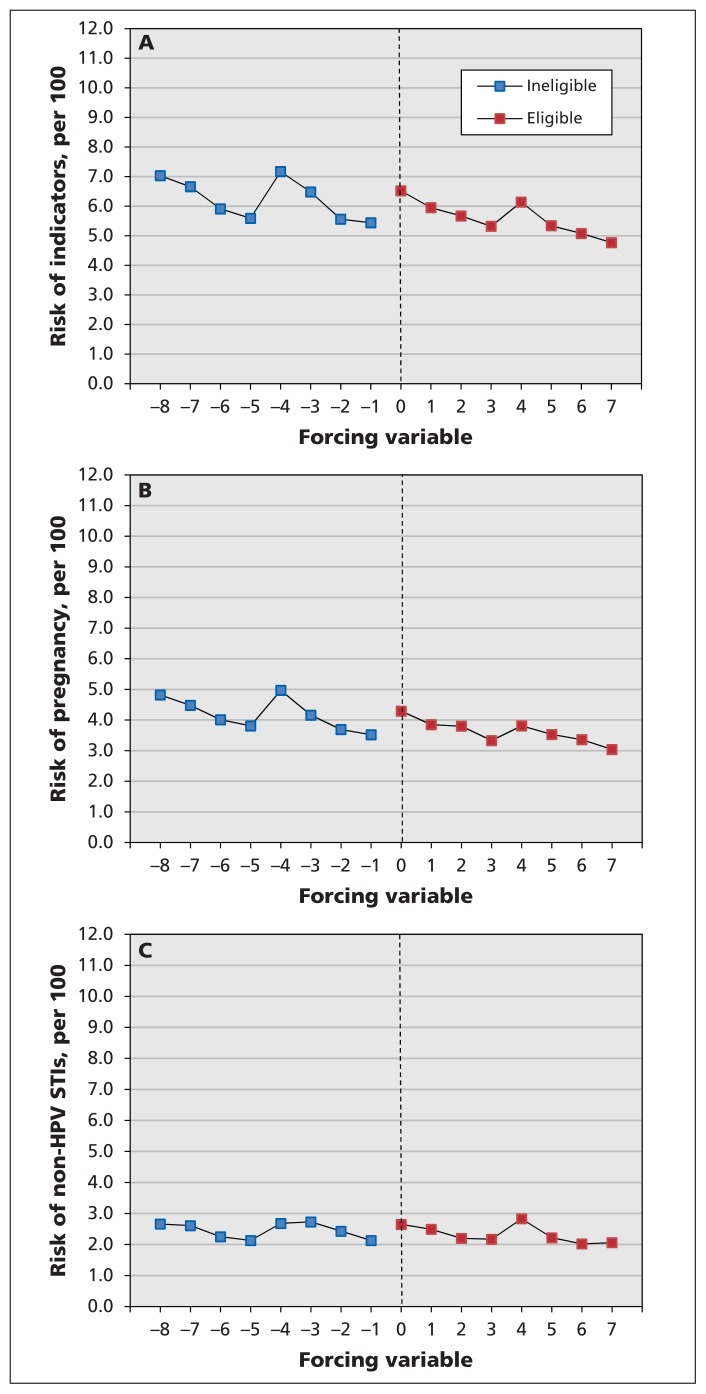
Results: The cohort comprised 260 493 girls, of whom 131 781 were ineligible for the program and 128 712 were eligible. We identified 15 441 (5.9%) cases of pregnancy and sexually transmitted infection and found no evidence that vaccination increased the risk of this composite outcome: RD per 1000 girls -0.61 (95% confidence interval [CI] -10.71 to 9.49) and RR 0.96 (95% CI 0.81 to 1.14). Similarly, we found no discernible effect of program eligibility: RD per 1000 girls -0.25 (95% CI -4.35 to 3.85) and RR 0.99 (95% CI 0.93 to 1.06). The findings were similar when outcomes were assessed separately.
Interpretation: We present strong evidence that HPV vaccination does not have any significant effect on clinical indicators of sexual behaviour among adolescent girls. These results suggest that concerns over increased promiscuity following HPV vaccination are unwarranted and should not deter from vaccinating at a young age.
© 2015 Canadian Medical Association or its licensors.
Figures
References
-
- Trottier H, Franco EL. The epidemiology of genital human papillomavirus infection. Vaccine 2006;24 Suppl 1:S1–15. - PubMed
-
- Muñoz N, Bosch FX, Castellsague X, et al. Against which human papillomavirus types shall we vaccinate and screen? The international perspective. Int J Cancer 2004;111:278–85. - PubMed
-
- Lacey CJ, Lowndes CM, Shah KV. Chapter 4: Burden and management of non-cancerous HPV-related conditions: HPV-6/11 disease. Vaccine 2006;24 Suppl 3:S3/35–41. - PubMed
-
- Haas M, Ashton T, Blum K, et al. Drugs, sex, money and power: an HPV vaccine case study. Health Policy 2009; 92:288–95. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous