

Selective Internal Radiation Therapy (SIRT) with yttrium-90 resin microspheres plus standard systemic chemotherapy regimen of FOLFOX versus FOLFOX alone as first-line treatment of non-resectable liver metastases from colorectal cancer: the SIRFLOX study
- PMID: 25487708
- PMCID: PMC4289171
- DOI: 10.1186/1471-2407-14-897
Selective Internal Radiation Therapy (SIRT) with yttrium-90 resin microspheres plus standard systemic chemotherapy regimen of FOLFOX versus FOLFOX alone as first-line treatment of non-resectable liver metastases from colorectal cancer: the SIRFLOX study
Abstract
Background: In colorectal cancer (CRC), unresectable liver metastases are linked to poor prognosis. Systemic chemotherapy with regimens such as FOLFOX (combination of infusional 5-fluorouracil, leucovorin and oxaliplatin) is the standard first-line treatment. The SIRFLOX trial was designed to assess the efficacy and safety of combining FOLFOX-based chemotherapy with Selective Internal Radiation Therapy (SIRT or radioembolisation) using yttrium-90 resin microspheres (SIR-SpheresR; Sirtex Medical Limited, North Sydney, Australia).
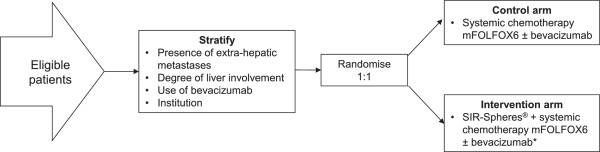
Methods/design: SIRFLOX is a randomised, multicentre trial of mFOLFOX6 chemotherapy+/-SIRT as first-line treatment of patients with liver-only or liver-predominant metastatic CRC (mCRC). The trial aims to recruit adult chemotherapy-naive patients with proven liver metastases with or without limited extra-hepatic disease, a life expectancy of >=3 months and a WHO performance status of 0-1. Patients will be randomised to receive either mFOLFOX6 or SIRT+mFOLFOX6 (with a reduced dose of oxaliplatin in cycles 1-3 following SIRT). Patients in both arms can receive bevacizumab at investigator discretion. Protocol chemotherapy will continue until there is unacceptable toxicity, evidence of tumour progression, complete surgical resection or ablation of cancerous lesions, or the patient requests an end to treatment. The primary endpoint of the SIRFLOX trial is progression-free survival (PFS). Secondary endpoints include: PFS in the liver; tumour response rate (liver and any site); site of tumour progression; health-related quality of life; toxicity and safety; liver resection rate; and overall survival. Assuming an increase in the median PFS from 9.4 months to 12.5 months with the addition of SIRT to mFOLFOX6, recruiting >=450 patients will be sufficient for 80% power and 95% confidence.
Discussion: The SIRFLOX trial will establish the potential role of SIRT+standard systemic chemotherapy in the first-line management of mCRC with non-resectable liver metastases.
Trial registration: SIRFLOX ClinicalTrials.gov identifier: NCT00724503. Registered 25 July 2008.
Figures

References
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2407/14/897/prepub
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
