

Added benefit of raxibacumab to antibiotic treatment of inhalational anthrax
- PMID: 25487792
- PMCID: PMC4335881
- DOI: 10.1128/AAC.04606-14
Added benefit of raxibacumab to antibiotic treatment of inhalational anthrax
Abstract
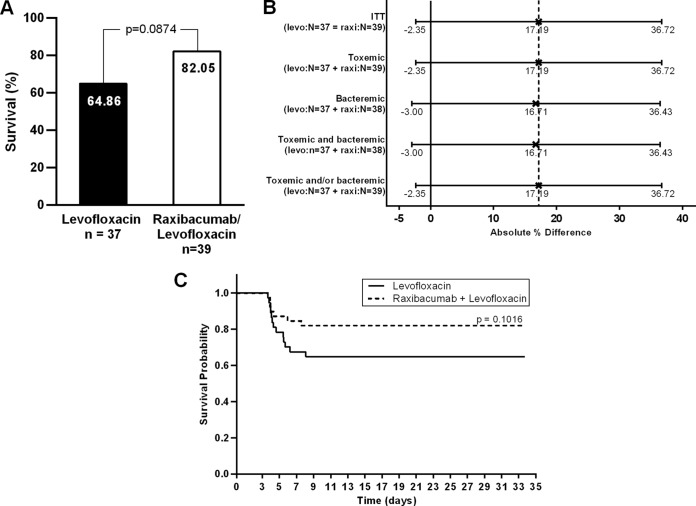
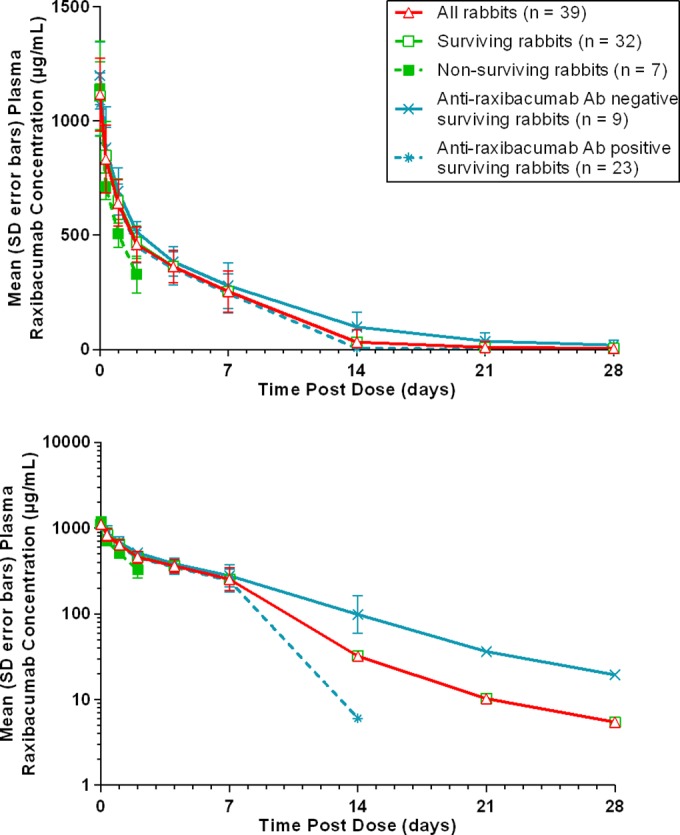
Although antibiotics treat bacteremia in inhalational anthrax, pathogenesis is mainly driven by bacterial exotoxins. Raxibacumab, an IgG1 monoclonal antibody, binds the protective antigen (PA) of Bacillus anthracis, thus blocking toxin effects and leading to improved survival in the rabbit and monkey models of inhalational anthrax. To assess raxibacumab's added benefit over levofloxacin (LVX) alone, rabbits surviving to 84 h after a challenge with 200 times the median (50%) lethal dose of B. anthracis spores were randomized to receive 3 daily intragastric LVX doses of 50 mg/kg of body weight, with the first LVX dose administered just prior to administration of a single intravenous dose of placebo or 40 mg/kg raxibacumab. The percentages of animals alive at 28 days following the last LVX dose were compared between the 2 treatment groups using a two-sided likelihood-ratio chi-square test. The 82% survival rate for the LVX-raxibacumab combination was higher than the 65% survival rate for LVX alone (P=0.0874). There were nearly 2-fold fewer deaths for the combination (7 deaths; n=39) than for LVX alone (13 deaths; n=37), and the survival time was prolonged for the combination (P=0.1016). Toxin-neutralizing-activity titers were similar for both treatment groups, suggesting that survivors in both groups were able to mount a toxin-neutralizing immune response. Microscopic findings considered consistent with anthrax were present in animals that died or became moribund on study in both treatment groups, and there were no anthrax-related findings in animals that survived. Overall, raxibacumab provided a meaningful benefit over antibiotic alone when administered late in the disease course.
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
Figures
Similar articles
-
Raxibacumab for the treatment of inhalational anthrax.N Engl J Med. 2009 Jul 9;361(2):135-44. doi: 10.1056/NEJMoa0810603. N Engl J Med. 2009. PMID: 19587338 Clinical Trial.
-
Bacillus anthracis protective antigen kinetics in inhalation spore-challenged untreated or levofloxacin/ raxibacumab-treated New Zealand white rabbits.Toxins (Basel). 2013 Jan 14;5(1):120-38. doi: 10.3390/toxins5010120. Toxins (Basel). 2013. PMID: 23344456 Free PMC article.
-
Raxibacumab for inhalational anthrax: an effective specific therapeutic approach?Expert Opin Investig Drugs. 2010 Jul;19(7):909-11. doi: 10.1517/13543784.2010.489547. Expert Opin Investig Drugs. 2010. PMID: 20450444
-
A Review of the Efficacy of FDA-Approved B. anthracis Anti-Toxin Agents When Combined with Antibiotic or Hemodynamic Support in Infection- or Toxin-Challenged Preclinical Models.Toxins (Basel). 2021 Jan 13;13(1):53. doi: 10.3390/toxins13010053. Toxins (Basel). 2021. PMID: 33450877 Free PMC article. Review.
-
Raxibacumab: potential role in the treatment of inhalational anthrax.Infect Drug Resist. 2014 Apr 29;7:101-9. doi: 10.2147/IDR.S47305. eCollection 2014. Infect Drug Resist. 2014. PMID: 24812521 Free PMC article. Review.
Cited by
-
Layered and integrated medical countermeasures against Burkholderia pseudomallei infections in C57BL/6 mice.Front Microbiol. 2022 Aug 17;13:965572. doi: 10.3389/fmicb.2022.965572. eCollection 2022. Front Microbiol. 2022. PMID: 36060756 Free PMC article.
-
Estimation of Time Period for Effective Human Inhalational Anthrax Treatment Including Antitoxin Therapy.PLoS Curr. 2017 Jul 28;9:ecurrents.outbreaks.7896c43f69838f17ce1c2c372e79d55d. doi: 10.1371/currents.outbreaks.7896c43f69838f17ce1c2c372e79d55d. PLoS Curr. 2017. PMID: 28856066 Free PMC article.
-
In Vivo Activity of Repurposed Amodiaquine as a Host-Targeting Therapy for the Treatment of Anthrax.ACS Infect Dis. 2021 Aug 13;7(8):2176-2191. doi: 10.1021/acsinfecdis.1c00190. Epub 2021 Jul 4. ACS Infect Dis. 2021. PMID: 34218660 Free PMC article.
-
Different mechanisms of two anti-anthrax protective antigen antibodies and function comparison between them.BMC Infect Dis. 2019 Nov 7;19(1):940. doi: 10.1186/s12879-019-4508-z. BMC Infect Dis. 2019. PMID: 31699037 Free PMC article.
-
Current Status and Trends in Prophylaxis and Management of Anthrax Disease.Pathogens. 2020 May 12;9(5):370. doi: 10.3390/pathogens9050370. Pathogens. 2020. PMID: 32408493 Free PMC article. Review.
References
-
- Inglesby TV, O'Toole T, Henderson DA, Bartlett JG, Ascher MS, Eitzen E, Friedlander AM, Gerberding J, Hauer J, Hughes J, McDade J, Osterholmn MT, Parker G, Perl TM, Russell PK, Tonat K. 2002. Anthrax as a biological weapon, 2002: updated recommendations for management. JAMA 287:2236–2252. doi:10.1001/jama.287.17.2236. - DOI - PubMed
-
- Jernigan DB, Raghunathan PL, Bell BP, Brechner R, Bresnitz EA, Butler JC, Cetron M, Cohen M, Doyle T, Fischer M, Greene C, Griffith KS, Guarner J, Hadler JL, Hayslett JA, Meyer R, Petersen LR, Phillips M, Pinner R, Popovic T, Quinn CP, Reefhuis J, Reissman D, Rosenstein N, Schuchat A, Shieh W-J, Siegal L, Swerdlow DL, Tenover FC, Traeger M, Ward JW, Weisfuse I, Wiersma S, Yewskey K, Zaki S, Ashford DA, Perkins BA, Ostroff S, Hughes J, Fleming D, Koplan JP, Gerberding JL, , National Anthrax Epidemiologic Investigation Team . 2002. Investigation of bioterrorism-related anthrax, United States, 2001: epidemiologic findings. Emerg Infect Dis 8:1019–1028. doi:10.3201/eid0810.020353. - DOI - PMC - PubMed
-
- Jernigan JA, Stephens DS, Ashford DA, Omenaca C, Topiel MS, Galbraith M, Tapper M, Fisk TL, Zaki S, Popovic T, Meyer RF, Quinn CP, Harper SA, Fridkin SK, Sejvar JJ, Shepard CW, McConnell M, Guarner J, Shieh W-J, Malecki JM, Gerberding JL, Hughes JM, Perkins BA, Members of the Anthrax Bioterrorism Investigation Team . 2001. Bioterrorism-related inhalational anthrax: the first 10 cases reported in the United States. Emerg Infect Dis 7:933–944. doi:10.3201/eid0706.010604. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
