

In-vivo assessment of the morphology and hemodynamic functions of the BioValsalva™ composite valve-conduit graft using cardiac magnetic resonance imaging and computational modelling technology
- PMID: 25488105
- PMCID: PMC4263057
- DOI: 10.1186/s13019-014-0193-6
In-vivo assessment of the morphology and hemodynamic functions of the BioValsalva™ composite valve-conduit graft using cardiac magnetic resonance imaging and computational modelling technology
Abstract
Background: The evaluation of any new cardiac valvular prosthesis should go beyond the classical morbidity and mortality rates and involve hemodynamic assessment. As a proof of concept, the objective of this study was to characterise for the first time the hemodynamics and the blood flow profiles at the aortic root in patients implanted with BioValsalva™ composite valve-conduit using comprehensive MRI and computer technologies.
Methods: Four male patients implanted with BioValsalva™ and 2 age-matched normal controls (NC) underwent cardiac magnetic resonance imaging (MRI). Phase-contrast imaging with velocity-mapping in 3 orthogonal directions was performed at the level of the aortic root and descending thoracic aorta. Computational fluid dynamic (CFD) simulations were performed for all the subjects with patient-specific flow information derived from phase-contrast MR data.
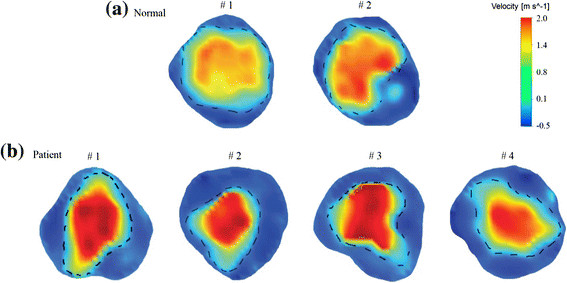
Results: The maximum and mean flow rates throughout the cardiac cycle at the aortic root level were very comparable between NC and BioValsalva™ patients (541 ± 199 vs. 567 ± 75 ml/s) and (95 ± 46 vs. 96 ± 10 ml/s), respectively. The maximum velocity (cm/s) was higher in patients (314 ± 49 vs. 223 ± 20; P = 0.06) due to relatively smaller effective orifice area (EOA), 2.99 ± 0.47 vs. 4.40 ± 0.24 cm2 (P = 0.06), however, the BioValsalva™ EOA was comparable to other reported prosthesis. The cross-sectional area and maximum diameter at the root were comparable between the two groups. BioValsalva™ conduit was stiffer than the native aortic wall, compliance (mm2 • mmHg(-1) • 10(-3)) values were (12.6 ± 4.2 vs 25.3 ± 0.4.; P = 0.06). The maximum time-averaged wall shear stress (Pa), at the ascending aorta was equivalent between the two groups, 17.17 ± 2.7 (NC) vs. 17.33 ± 4.7 (BioValsalva™ ). Flow streamlines at the root and ascending aorta were also similar between the two groups apart from a degree of helical flow that occurs at the outer curvature at the angle developed near the suture line.
Conclusions: BioValsalva™ composite valve-conduit prosthesis is potentially comparable to native aortic root in structural design and in many hemodynamic parameters, although it is stiffer. Surgeons should pay more attention to the surgical technique to maximise the reestablishment of normal smooth aortic curvature geometry to prevent unfavourable flow characteristics.
Figures





Similar articles
-
Assessment of Hemodynamic Conditions in the Aorta Following Root Replacement with Composite Valve-Conduit Graft.Ann Biomed Eng. 2016 May;44(5):1392-404. doi: 10.1007/s10439-015-1453-x. Epub 2015 Sep 14. Ann Biomed Eng. 2016. PMID: 26369636 Clinical Trial.
-
Hemodynamic Evaluation of a Biological and Mechanical Aortic Valve Prosthesis Using Patient-Specific MRI-Based CFD.Artif Organs. 2018 Jan;42(1):49-57. doi: 10.1111/aor.12955. Epub 2017 Aug 29. Artif Organs. 2018. PMID: 28853220
-
Patient-specific computational fluid dynamics-assessment of aortic hemodynamics in a spectrum of aortic valve pathologies.J Thorac Cardiovasc Surg. 2017 Jan;153(1):8-20.e3. doi: 10.1016/j.jtcvs.2016.09.040. Epub 2016 Sep 23. J Thorac Cardiovasc Surg. 2017. PMID: 27847162
-
Four-dimensional-flow Magnetic Resonance Imaging of the Aortic Valve and Thoracic Aorta.Radiol Clin North Am. 2020 Jul;58(4):753-763. doi: 10.1016/j.rcl.2020.02.008. Epub 2020 May 12. Radiol Clin North Am. 2020. PMID: 32471542 Review.
-
[MR-based tridirectional flow imaging. Acquisition and 3D analysis of flows in the thoracic aorta].Radiologe. 2007 Nov;47(11):1012-20. doi: 10.1007/s00117-007-1577-6. Radiologe. 2007. PMID: 17932640 Review. German.
Cited by
-
Ultrasound imaging velocimetry with interleaved images for improved pulsatile arterial flow measurements: a new correction method, experimental and in vivo validation.J R Soc Interface. 2017 Feb;14(127):20160761. doi: 10.1098/rsif.2016.0761. J R Soc Interface. 2017. PMID: 28148767 Free PMC article.
-
Old Myths, New Concerns: the Long-Term Effects of Ascending Aorta Replacement with Dacron Grafts. Not All That Glitters Is Gold.J Cardiovasc Transl Res. 2016 Aug;9(4):334-42. doi: 10.1007/s12265-016-9699-8. Epub 2016 May 31. J Cardiovasc Transl Res. 2016. PMID: 27245785 Free PMC article. Review.
-
Perioperative evaluation of regional aortic wall shear stress patterns in patients undergoing aortic valve and/or proximal thoracic aortic replacement.J Thorac Cardiovasc Surg. 2018 Jun;155(6):2277-2286.e2. doi: 10.1016/j.jtcvs.2017.11.007. Epub 2017 Nov 16. J Thorac Cardiovasc Surg. 2018. PMID: 29248286 Free PMC article.
References
-
- Hagl C, Strauch JT, Spielvogel D, Galla JD, Lansman SL, Squitieri R, Bodian CA, Griepp RB. Is the Bentall procedure for ascending aorta or aortic valve replacement the best approach for long-term event-free survival? Ann Thorac Surg. 2003;76:698–703. doi: 10.1016/S0003-4975(03)00568-X. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
