

Risk factors for acute kidney injury in older adults with critical illness: a retrospective cohort study
- PMID: 25488106
- PMCID: PMC4442750
- DOI: 10.1053/j.ajkd.2014.10.018
Risk factors for acute kidney injury in older adults with critical illness: a retrospective cohort study
Abstract
Background: Risk for acute kidney injury (AKI) in older adults has not been evaluated systematically. We sought to delineate the determinants of risk for AKI in older compared with younger adults.
Study design: Retrospective analysis of patients hospitalized in July 2000 to September 2008.
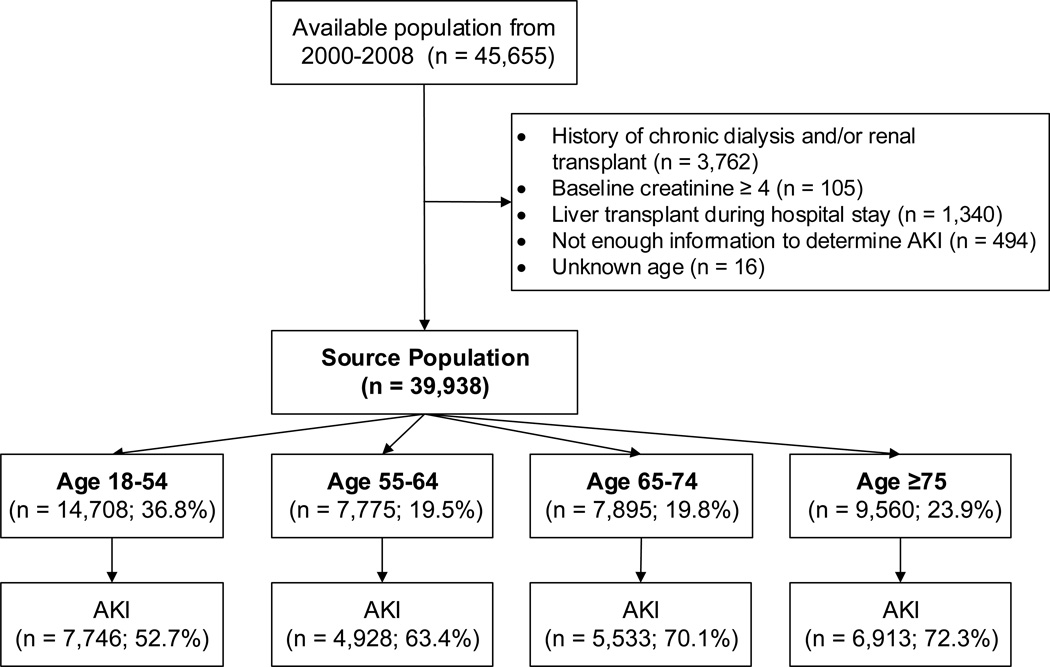
Setting & participants: We identified all adult patients admitted to an intensive care unit (n=45,655) in a large tertiary-care university hospital system. We excluded patients receiving dialysis or a kidney transplant prior to hospital admission and patients with baseline creatinine levels ≥ 4mg/dL, liver transplantation, indeterminate AKI status, or unknown age, leaving 39,938 patients.
Predictor: We collected data for multiple susceptibilities and exposures, including age, sex, race, body mass, comorbid conditions, severity of illness, baseline kidney function, sepsis, and shock.
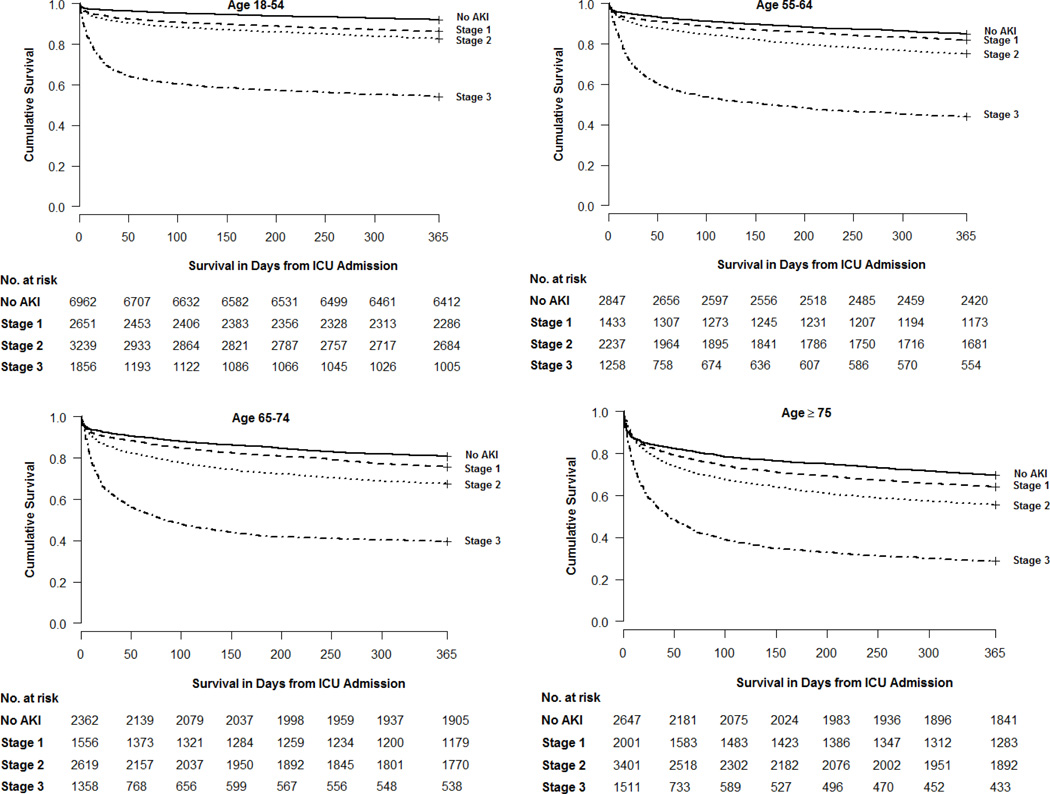
Outcomes: We defined AKI according to KDIGO (Kidney Disease: Improving Global Outcomes) criteria. We examined susceptibilities and exposures across age strata for impact on the development of AKI.
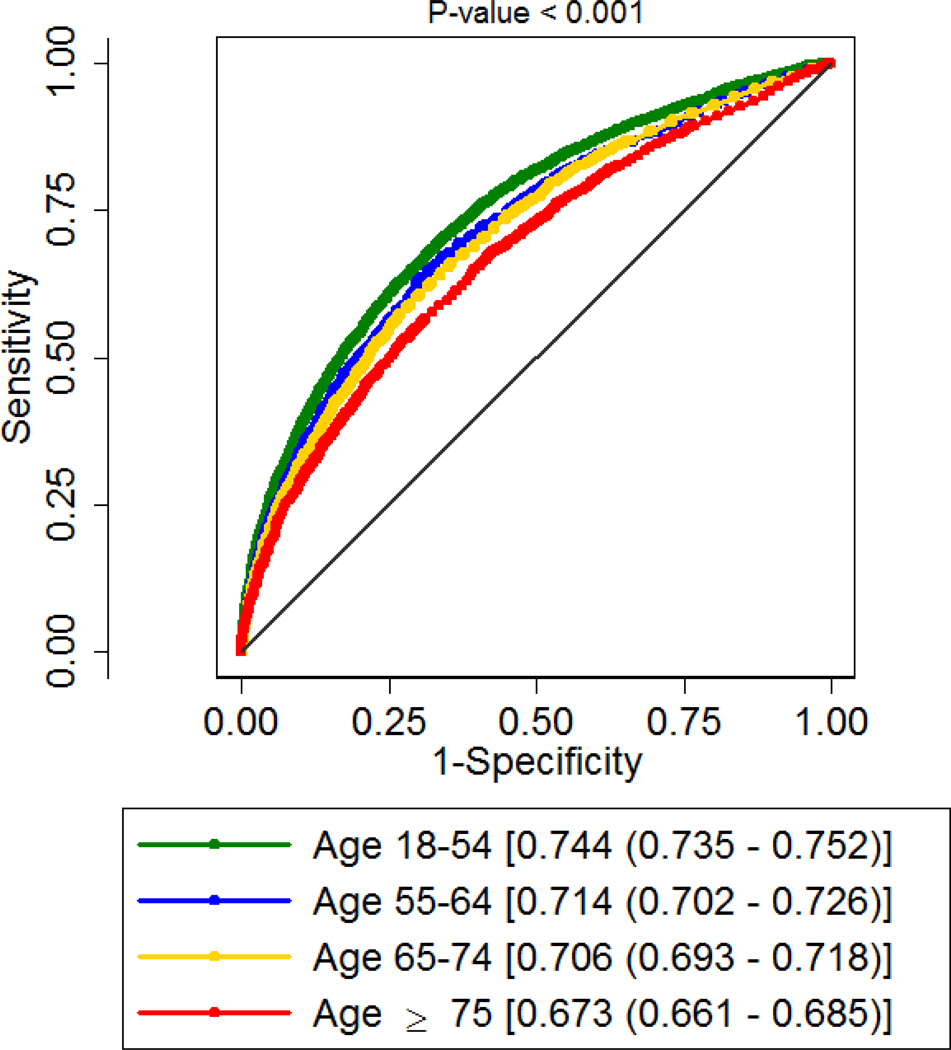
Measurements: We calculated area under the receiver operating characteristic curve (AUC) for prediction of AKI across age groups.
Results: 25,230 (63.2%) patients were 55 years or older. Overall, 25,120 (62.9%) patients developed AKI (69.2% aged ≥55 years). Examples of risk factors for AKI in the oldest age category (≥75 years) were drugs (vancomycin, aminoglycosides, and nonsteroidal anti-inflammatories), history of hypertension (OR, 1.13; 95% CI, 1.02-1.25), and sepsis (OR, 2.12; 95% CI, 1.68-2.67). Fewer variables remained predictive of AKI as age increased and the model for older patients was less predictive (P<0.001). For the age categories 18 to 54, 55 to 64, 65 to 74, and 75 years or older, AUCs were 0.744 (95% CI, 0.735-0.752), 0.714 (95% CI, 0.702-0.726), 0.706 (95% CI, 0.693-0.718), and 0.673 (95% CI, 0.661-0.685), respectively.
Limitations: Analysis may not apply to non-intensive care unit patients.
Conclusions: The likelihood of developing AKI increases with age; however, the same variables are less predictive for AKI as age increases. Efforts to quantify risk for AKI may be more difficult in older adults.
Keywords: Acute kidney injury (AKI); age; chronic kidney disease (CKD); critical illness; elderly; intensive care unit (ICU); older; risk; risk prediction; susceptibilities and exposures.
Copyright © 2015 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Fischer MJ, Brimhall BB, Lezotte DC, Glazner Je, Parikh CR. Uncomplicated acute renal failure and hospital resource utilization: a retrospective multicenter analysis. Am J Kidney Dis. 2005;46(6):1049–1057. - PubMed
-
- Uchino S, Bellomo R, Goldsmith D, Bates S, Ronco C. An assessment of the RIFLE criteria for acute renal failure in hospitalized patients. Crit Care Med. 2006;34(7):1913-. - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO)Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
