

The EQ-5D-5L Improves on the EQ-5D-3L for Health-related Quality-of-life Assessment in Patients Undergoing Total Hip Arthroplasty
- PMID: 25488404
- PMCID: PMC4586224
- DOI: 10.1007/s11999-014-4091-y
The EQ-5D-5L Improves on the EQ-5D-3L for Health-related Quality-of-life Assessment in Patients Undergoing Total Hip Arthroplasty
Abstract
Background: The EQ-5D is a generic health survey that can be used to compare improvement across different interventions, measure changes in health-related quality of life over time, or to explore cost-effectiveness among treatments, hospitals, or providers. The original EQ-5D survey has three response options for each of five health dimensions; however, with so few response options, ceiling and floor effects are problematic in some populations. A new version, called the EQ-5D-5L, was developed, which gives respondents five answer options (the "5L" refers to five response levels, which is in contrast to the original survey's three levels). However, the validity of this version has not, to our knowledge, been evaluated in patients undergoing total hip arthroplasty (THA).
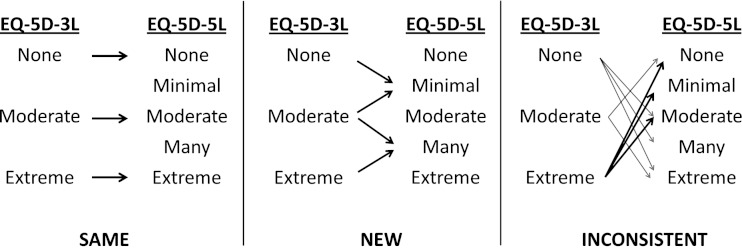
Questions/purposes: The purposes of this study were (1) to characterize the redistribution of responses using the new version; (2) to describe the ceiling and floor effects in the current three-level version and identify whether the new EQ-5D-5L survey diminished these effects; and (3) to understand the convergent validity of the new version with the old and the EQ visual analog scale.
Methods: Both versions of the survey were administered either preoperatively or 1 to 6 years after THA, allowing at least 2 weeks between administrations. Responses to the two versions were compared to determine response redistribution properties, ceiling and floor effects, and convergent validity. Sample sizes were determined so that the study would have 90% power to detect a Spearman correlation over 0.7 when comparing the responses of the three-level survey with the five-level survey and allowing for a rate of 25% loss to followup.
Results: Most patients before surgery used the new responses in the majority of dimensions, whereas the patients taking the test after surgery used the new responses predominantly for the pain dimension. The five-level diminished ceiling effects in both groups by up to 30% and diminished floor effects in the pain dimension for patients taking the assessment before surgery by 14%, which was the only dimension in either patient group that had high rates of floor effects. The correlation between the surveys' visual analog scale and response patterns was not different for the two versions of the survey in these populations.
Conclusions: The EQ-5D five-level survey appears able to discriminate new health states indistinguishable in the original, which may allow more sensitive measurements of change in patients undergoing THA. The five-level survey should be considered for implementation in local and national registry monitoring of health-related quality of life in patients undergoing THA.
Figures

Comment in
-
Patient-reported outcome measures in arthroplasty registries Report of the Patient-Reported Outcome Measures Working Group of the International Society of Arthroplasty Registries Part II. Recommendations for selection, administration, and analysis.Acta Orthop. 2016 Jul;87 Suppl 1(Suppl 1):9-23. doi: 10.1080/17453674.2016.1181816. Epub 2016 May 26. Acta Orthop. 2016. PMID: 27228230 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
