

Hemodynamic-morphological discriminant models for intracranial aneurysm rupture remain stable with increasing sample size
- PMID: 25488922
- PMCID: PMC4791310
- DOI: 10.1136/neurintsurg-2014-011477
Hemodynamic-morphological discriminant models for intracranial aneurysm rupture remain stable with increasing sample size
Abstract
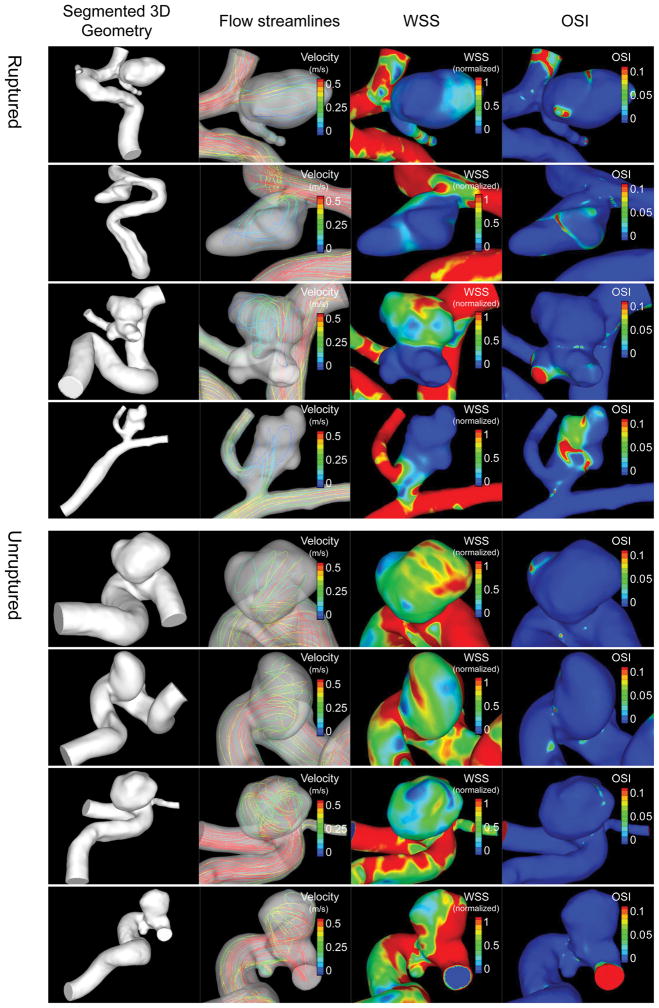
Background: We previously established three logistic regression models for discriminating intracranial aneurysm rupture status based on morphological and hemodynamic analysis of 119 aneurysms. In this study, we tested if these models would remain stable with increasing sample size, and investigated sample sizes required for various confidence levels (CIs).
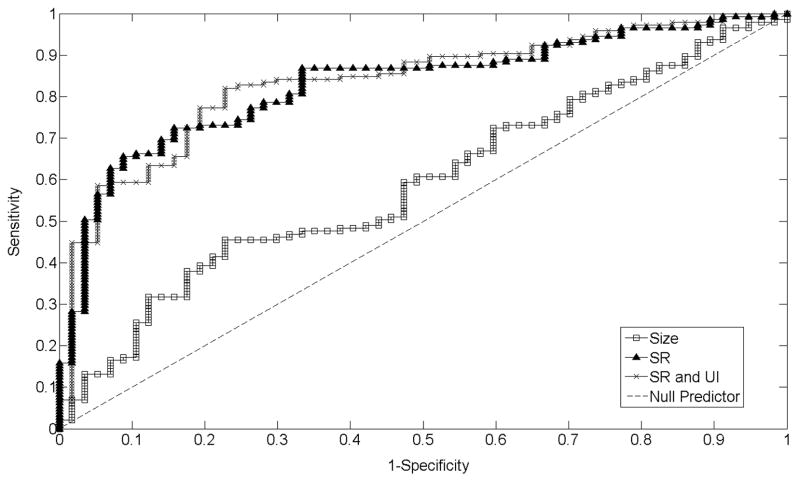
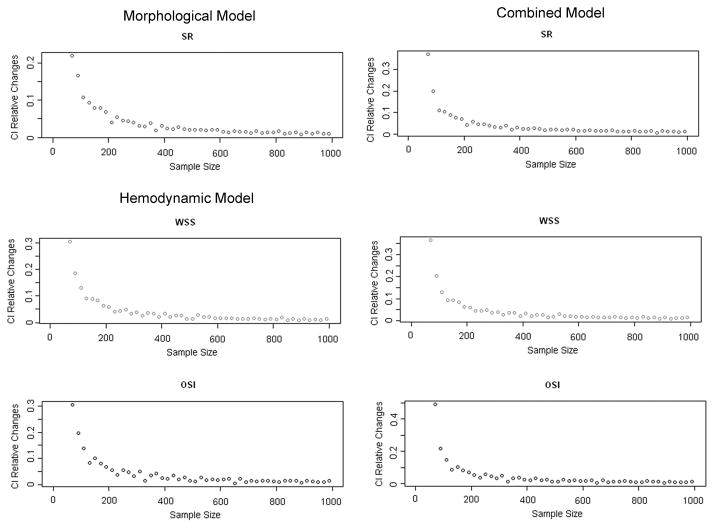
Methods: We augmented our previous dataset of 119 aneurysms into a new dataset of 204 samples by collecting an additional 85 consecutive aneurysms, on which we performed flow simulation and calculated morphological and hemodynamic parameters, as done previously. We performed univariate significance tests on these parameters, and multivariate logistic regression on significant parameters. The new regression models were compared against the original models. Receiver operating characteristics analysis was applied to compare the performance of regression models. Furthermore, we performed regression analysis based on bootstrapping resampling statistical simulations to explore how many aneurysm cases were required to generate stable models.
Results: Univariate tests of the 204 aneurysms generated an identical list of significant morphological and hemodynamic parameters as previously (from the analysis of 119 cases). Furthermore, multivariate regression analysis produced three parsimonious predictive models that were almost identical to the previous ones, with model coefficients that had narrower CIs than the original ones. Bootstrapping showed that 10%, 5%, 2%, and 1% convergence levels of CI required 120, 200, 500, and 900 aneurysms, respectively.
Conclusions: Our original hemodynamic-morphological rupture prediction models are stable and improve with increasing sample size. Results from resampling statistical simulations provide guidance for designing future large multi-population studies.
Keywords: Aneurysm; Blood Flow; Stroke.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Conflict of interest statement
Dr. Xiang: recipient of Dr. Richard J. Schlesinger grant from the American Society for Quality Biomedical Biomedical Division and principal investigator of Dawn Brejcha Chair of Research grant from Brain Aneurysm Foundation.
Dr. Yu: none.
Dr. Snyder: consultant: Toshiba; speakers’ bureau: Toshiba, ev3/Covidien and The Stroke Group; honoraria: Toshiba, ev3/Covidien and The Stroke Group.
Dr. Levy: shareholder/ownership interests: Intratech Medical Ltd., Mynx/Access Closure, Blockade Medical LLC. Principal investigator: Covidien US SWIFT PRIME Trials. Other financial support: Abbott for carotid training for physicians.
Dr. Siddiqui: research grants: co-investigator of NIH grants (R01NS064592 and 5R01EB002873) and Research Development Award from the University at Buffalo; financial interests: Blockade Medical, Hotspur, Intratech Medical, Lazarus Effect, StimSox, Valor Medical; consultant: Blockade Medical, Codman & Shurtleff, Inc., Concentric Medical, ev3/Covidien Vascular Therapies, GuidePoint Global Consulting, Lazarus Effect, MicroVention, Penumbra, Stryker, Pulsar Vascular; National Steering Committee: 3D Separator Trial (Penumbra, Inc.), SWIFT PRIME Trial (Covidien), FRED Trial (MicroVention); speakers’ bureau: Codman & Shurtleff, Inc.; advisory board: Codman & Shurtleff, Inc., Covidien Neurovascular; honoraria: Abbott Vascular and Codman & Shurtleff, Inc. for training other physicians in carotid stenting and endovascular stenting for aneurysms, and Penumbra, Inc.
Dr. Meng: principal investigator of NIH grant (R01NS064592), the grant from Toshiba Medical Systems and The Carol W. Harvey Memorial Chair of Research grant from Brain Aneurysm Foundation.
Figures


References
-
- Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: A systematic review. Stroke; a journal of cerebral circulation. 1998;29:251–256. - PubMed
-
- Cross DT, 3rd, Tirschwell DL, Clark MA, Tuden D, Derdeyn CP, Moran CJ, et al. Mortality rates after subarachnoid hemorrhage: Variations according to hospital case volume in 18 states. J Neurosurg. 2003;99:810–817. - PubMed
-
- Ujiie H, Tachibana H, Hiramatsu O, Hazel AL, Matsumoto T, Ogasawara Y, et al. Effects of size and shape (aspect ratio) on the hemodynamics of saccular aneurysms: A possible index for surgical treatment of intracranial aneurysms. Neurosurgery. 1999;45:119–130. - PubMed
-
- Raghavan ML, Ma B, Harbaugh RE. Quantified aneurysm shape and rupture risk. J Neurosurg. 2005;102:355–362. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical