

Institutional clinical trial accrual volume and survival of patients with head and neck cancer
- PMID: 25488965
- PMCID: PMC4279235
- DOI: 10.1200/JCO.2014.56.5218
Institutional clinical trial accrual volume and survival of patients with head and neck cancer
Abstract
Purpose: National Comprehensive Cancer Network guidelines recommend patients with head and neck cancer (HNC) receive treatment at centers with expertise, but whether provider experience affects survival is unknown.
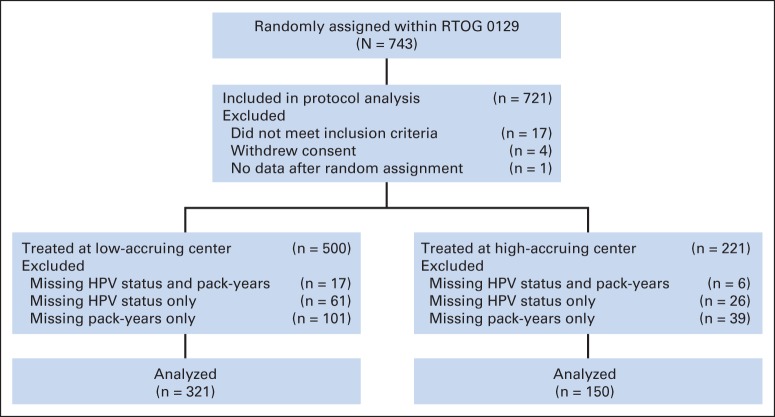
Patients and methods: The effect of institutional experience on overall survival (OS) in patients with stage III or IV HNC was investigated within a randomized trial of the Radiation Therapy Oncology Group (RTOG 0129), which compared cisplatin concurrent with standard versus accelerated fractionation radiotherapy. As a surrogate for experience, institutions were classified as historically low- (HLACs) or high-accruing centers (HHACs) based on accrual to 21 RTOG HNC trials (1997 to 2002). The effect of accrual volume on OS was estimated by Cox proportional hazards models.
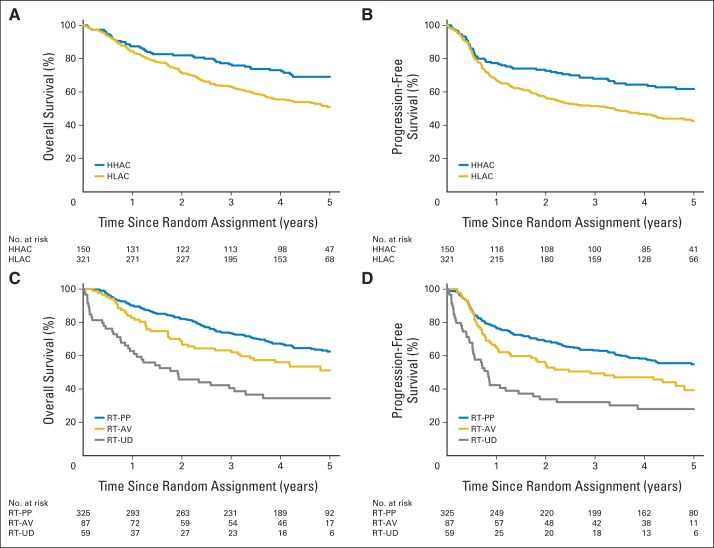
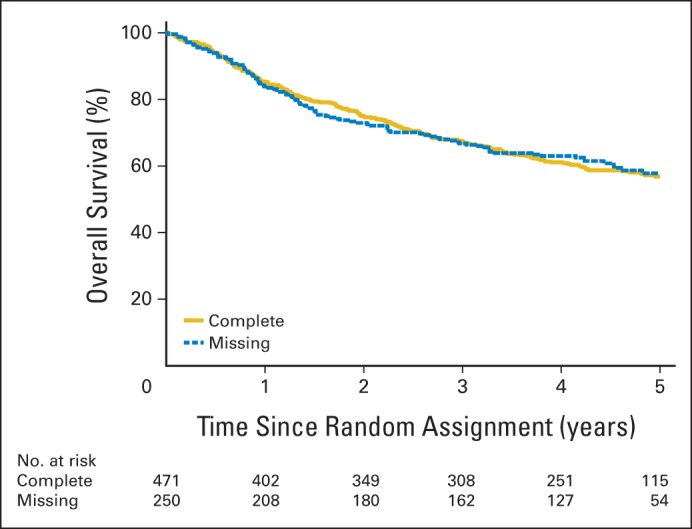
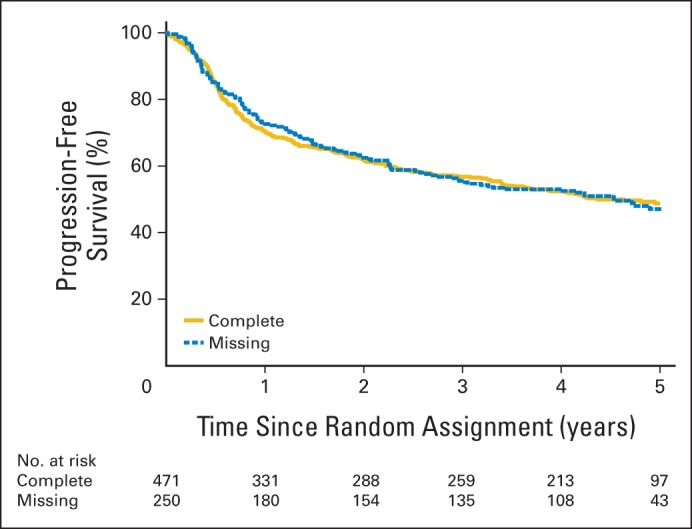
Results: Median RTOG accrual (1997 to 2002) at HLACs was four versus 65 patients at HHACs. Analysis included 471 patients in RTOG 0129 (2002 to 2005) with known human papillomavirus and smoking status. Patients at HLACs versus HHACs had better performance status (0: 62% v 52%; P = .04) and lower T stage (T4: 26.5% v 35.3%; P = .002) but were otherwise similar. Radiotherapy protocol deviations were higher at HLACs versus HHACs (18% v 6%; P < .001). When compared with HHACs, patients at HLACs had worse OS (5 years: 51.0% v 69.1%; P = .002). Treatment at HLACs was associated with increased death risk of 91% (hazard ratio [HR], 1.91; 95% CI, 1.37 to 2.65) after adjustment for prognostic factors and 72% (HR, 1.72; 95% CI, 1.23 to 2.40) after radiotherapy compliance adjustment.
Conclusion: OS is worse for patients with HNC treated at HLACs versus HHACs to cooperative group trials after accounting for radiotherapy protocol deviations. Institutional experience substantially influences survival in locally advanced HNC.
Trial registration: ClinicalTrials.gov NCT00047008.
© 2014 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
Impact of center size and experience on outcomes in head and neck cancer.J Clin Oncol. 2015 Jan 10;33(2):138-40. doi: 10.1200/JCO.2014.58.2239. Epub 2014 Dec 8. J Clin Oncol. 2015. PMID: 25488964 No abstract available.
References
-
- Luchtenborg M, Riaz SP, Coupland VH, et al. High procedure volume is strongly associated with improved survival after lung cancer surgery. J Clin Oncol. 2013;31:3141–3146. - PubMed
-
- Begg CB, Cramer LD, Hoskins WJ, et al. Impact of hospital volume on operative mortality for major cancer surgery. JAMA. 1998;280:1747–1751. - PubMed
-
- Bilimoria KY, Talamonti MS, Sener SF, et al. Effect of hospital volume on margin status after pancreaticoduodenectomy for cancer. J Am Coll Surg. 2008;207:510–519. - PubMed
-
- Birkmeyer JD, Finlayson SR, Tosteson AN, et al. Effect of hospital volume on in-hospital mortality with pancreaticoduodenectomy. Surgery. 1999;125:250–256. - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128–1137. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
