

Feasibility and acceptance of a robotic surgery ergonomic training program
- PMID: 25489213
- PMCID: PMC4254477
- DOI: 10.4293/JSLS.2014.00166
Feasibility and acceptance of a robotic surgery ergonomic training program
Abstract
Background and objectives: Assessment of ergonomic strain during robotic surgery indicates there is a need for intervention. However, limited data exist detailing the feasibility and acceptance of ergonomic training (ET) for robotic surgeons. This prospective, observational pilot study evaluates the implementation of an evidence-based ET module.
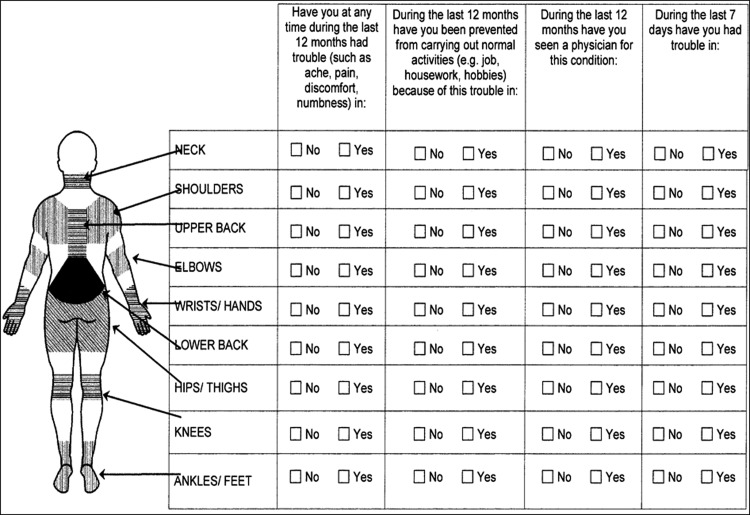
Methods: A two-part survey was conducted. The first survey assessed robotic strain using the Nordic Musculoskeletal Questionnaire (NMQ). Participants were given the option to participate in either an online or an in-person ET session. The ET was derived from Occupational Safety and Health Administration guidelines and developed by a human factors engineer experienced with health care ergonomics. After ET, a follow-up survey including the NMQ and an assessment of the ET were completed.
Results: The survey was sent to 67 robotic surgeons. Forty-two (62.7%) responded, including 18 residents, 8 fellows, and 16 attending physicians. Forty-five percent experienced strain resulting from performing robotic surgery and 26.3% reported persistent strain. Only 16.6% of surgeons reported prior ET in robotic surgery. Thirty-five (78%) surgeons elected to have in-person ET, which was successfully arranged for 32 surgeons (91.4%). Thirty-seven surgeons (88.1%) completed the follow-up survey. All surgeons participating in the in-person ET found it helpful and felt formal ET should be standard, 88% changed their practice as a result of the training, and 74% of those reporting strain noticed a decrease after their ET.
Conclusion: Thus, at a high-volume robotics center, evidence-based ET was easily implemented, well-received, changed some surgeons' practice, and decreased self-reported strain related to robotic surgery.
Keywords: Ergonomic strain; Ergonomic training; Robotic surgery; Strain.
Figures
References
-
- Wexner SD, Bergamaschi R, Lacy A, et al. The current status of robotic pelvic surgery: results of a multinational interdisciplinary consensus conference. Surg Endosc. 2009;23:438–443. - PubMed
-
- Challacombe BJ, Khan MS, Murphy D, Dasgupta P. The history of robotics in urology. World J Urol. 2006;24:120–127. - PubMed
-
- Ballantyne GH, Moll F. The da Vinci telerobotic surgical system: the virtual operative field and telepresence surgery. Surg Clin North Am 2003;83:1293–1304. - PubMed
-
- Mohr CJ, Nadzam GS, Curet MJ. Totally robotic Roux-en-Y gastric bypass. Arch Surg. 2005;140:779–786. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical