

Can we add auricular composite graft to our rhinoplasty armamentarium?
- PMID: 25489502
- PMCID: PMC4238327
Can we add auricular composite graft to our rhinoplasty armamentarium?
Abstract
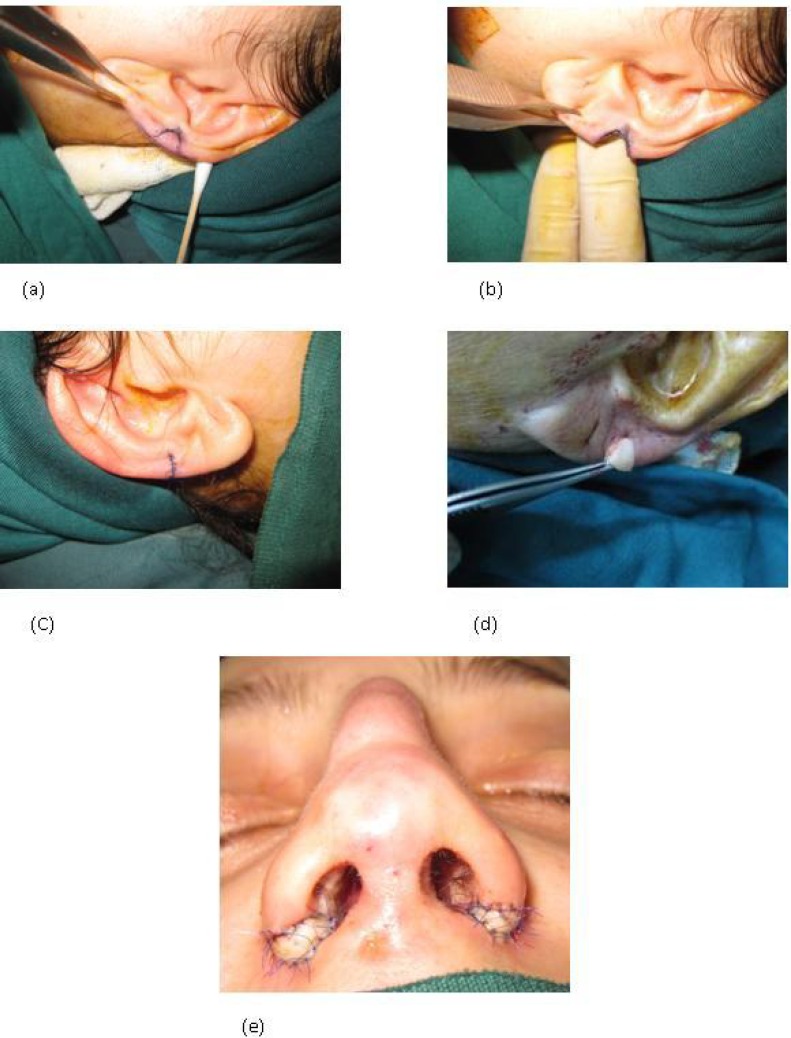
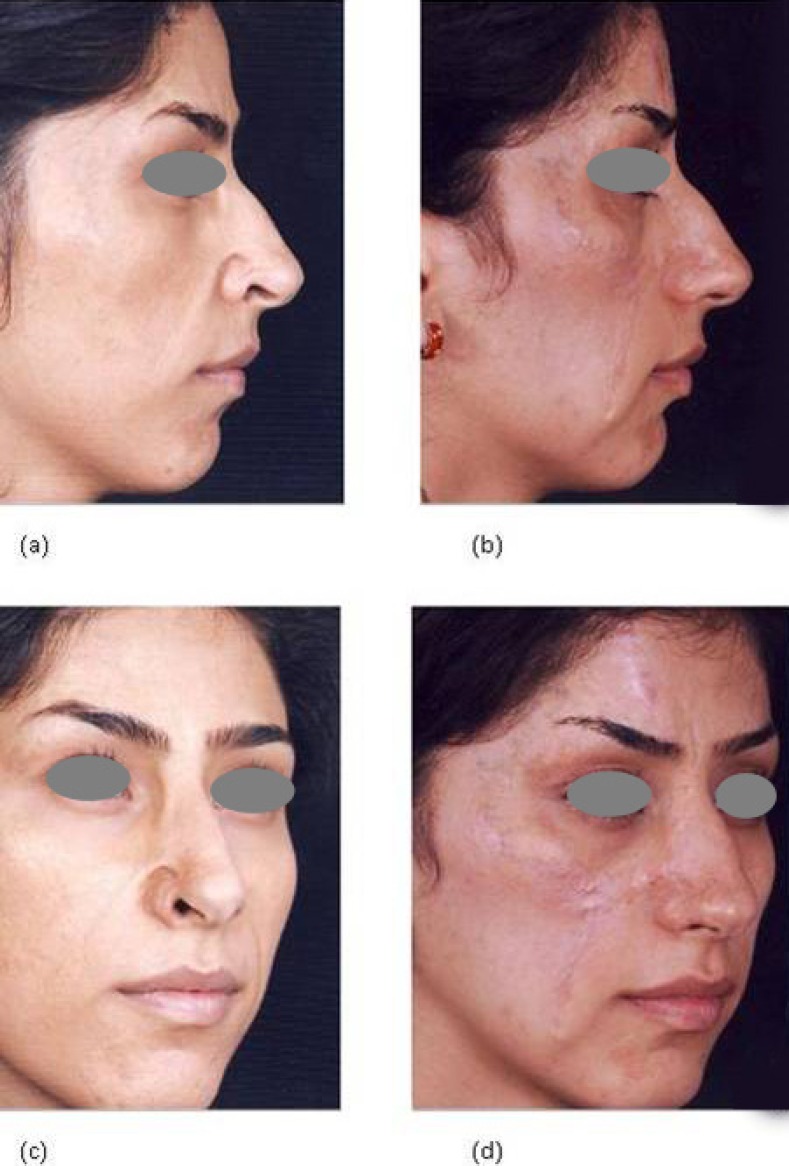
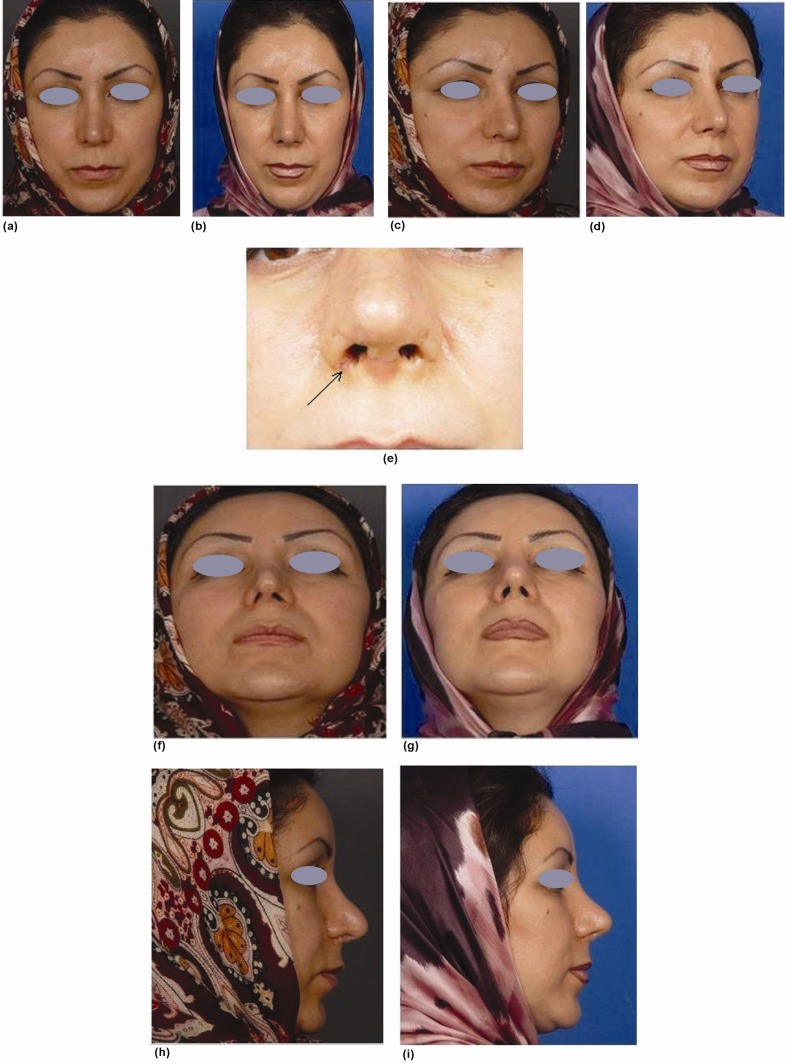
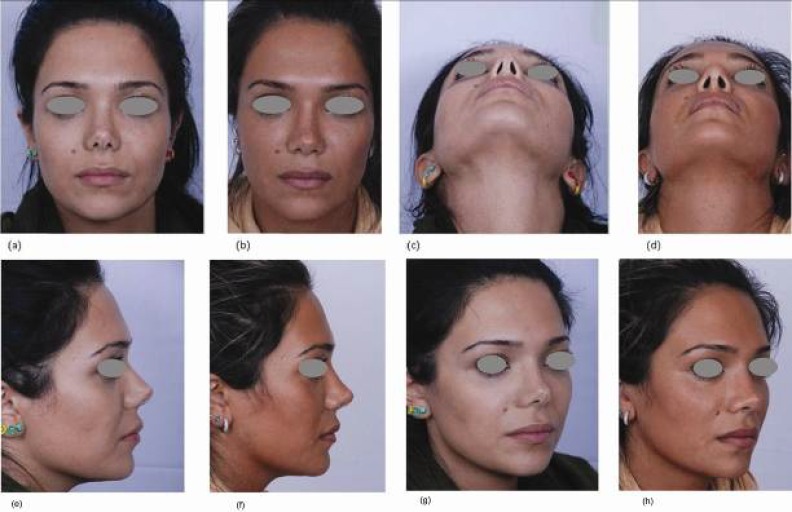
Background: The ala of the nose, with its particular texture and characteristics, poses both aesthetically and functionally intriguing challenges and is rather problematic regarding choices for reconstructive methods. Both flaps and grafts have been used to restore natural structure of nasal ala. The present study summarizes a ten-year experience of reconstructive surgery using small composite grafts from non-cartilage bearing tissues, and large composite grafts, containing cartilaginous tissue, with a mean follow-up of 4 years and 8 months.
Methods: Cumulatively 56 patients were reported. Some of them required surgery due to previous cosmetic rhinoplasty. In 47 of the cases, a small graft from the non-cartilage bearing junction of ear lobule to helical rim sufficed. Nine patients had rather large defects for which grafts were harvested from the helical root. Donor sites were primarily closed and grafts were implanted in place in a single, rapid session.
Results: All small grafts had excellent take. Of 9 large grafts, 5 had excellent take, three had acceptable, and one, in a male smoker, failed to take. During follow-up, no gross deformity or poor scar was detected in either donor or recipient site.
Conclusions: We have demonstrated that using both large and small auricular composite grafts has favorable long term results for reconstruction of alar rim deformities. However, use of small grafts seems more beneficial and applicability of large grafts requires further studies.
Keywords: Alar rim; Armamentarium; Auricular composite; Graft; Reconstruction; Rhinoplasty.
Figures

References
-
- Robinson JK, Burget , GC Nasal valve malfunction resulting from resection of cancer. Arch. Otolaryngol. Head Neck Surg. 1990;116:1419–24. - PubMed
-
- Constantian MB. The incompetent external nasal valve: Pathophysiology and treatment in primary and secondary rhinoplasty. Plast Reconstr Surg. 1994;93:919–31. - PubMed
-
- Sheen JH, Sheen AP. Aesthetic Rhinoplasty. 2nd Ed. St. Louis: Mosby; 1987. pp. 106–110.
-
- Sheen JH, Sheen AP. Aesthetic Rhinoplasty. 2nd Ed. St. Louis: Mosby; 1987. pp. 988–1011.
-
- Dupertuis SM. Free ear lobe grafts of skin and fat. Plast Reconstr Surg. 1945;1:135–44. - PubMed
LinkOut - more resources
Full Text Sources