

Prognostic value of high-sensitivity troponin T levels in patients with ventricular arrhythmias and out-of-hospital cardiac arrest: data from the prospective FINNRESUSCI study
- PMID: 25490117
- PMCID: PMC4256726
- DOI: 10.1186/s13054-014-0605-y
Prognostic value of high-sensitivity troponin T levels in patients with ventricular arrhythmias and out-of-hospital cardiac arrest: data from the prospective FINNRESUSCI study
Abstract
Introduction: Myocardial dysfunction is common after out-of-hospital cardiac arrest (OHCA) and high-sensitivity troponin T (hs-TnT) levels may provide incremental prognostic information to established risk indices.
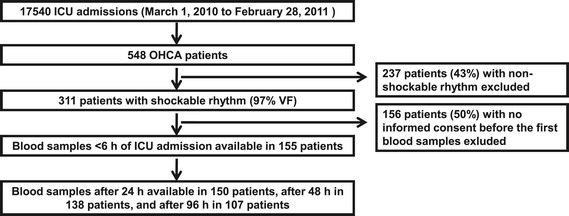
Methods: A total of 155 patients with OHCA and a shockable rhythm (98% ventricular fibrillation; OHCA-VF/VT) had blood samples drawn within six hours of admission. Blood samples were also available after 24 hours, 48 hours, and 96 hours in subsets of patients. The endpoints of the study were hospital mortality and neurological status and mortality after one year.
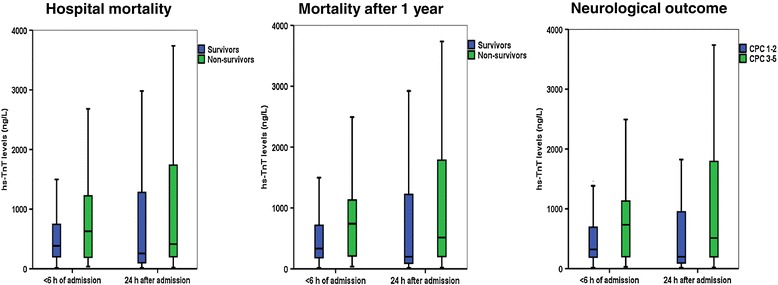
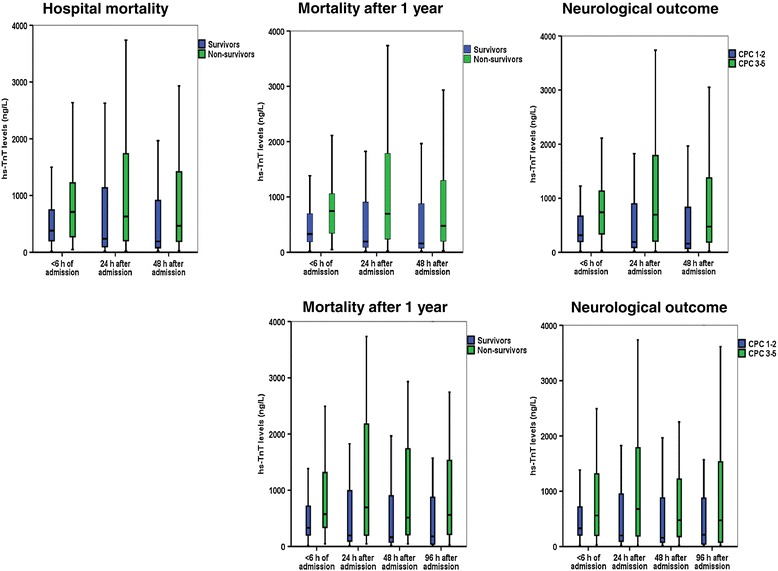
Results: Admission hs-TnT levels were higher than the 99-percentile of the general population (14 ng/L) in all patients (range 18 to 17,837 ng/L). Admission hs-TnT levels were associated with acute coronary artery occlusion, time to return of spontaneous circulation, heart failure, and renal function. Admission hs-TnT levels were higher in one-year non-survivors compared to survivors (median 747 (quartile 1 to 3, 206 to 1061) ng/L versus 345 (184 to 740) ng/L, P =0.023) and in patients with a poor versus a favorable neurological outcome (739 (191 to 1061) ng/L versus 334 (195 to 716) ng/L, P =0.028). However, hs-TnT measurements did not add prognostic information to established risk variables in multivariate analyses. hs-TnT levels measured during the hospitalization for OHCA-VF/VT correlated closely with admission levels (r ≥0.63) and were inferior to Simplified Acute Physiology Score II (SAPS II) scores for the prediction of events during follow-up. hs-TnT dynamics did not discriminate between survivors and non-survivors or between a poor versus a favorable neurological outcome.
Conclusion: hs-TnT levels are elevated in critically ill patients with OHCA-VF/VT, but do not improve risk prediction.
Figures
References
-
- Stiell IG, Wells GA, Field B, Spaite DW, Nesbitt LP, De Maio VJ, Nichol G, Cousineau D, Blackburn J, Munkley D, Luinstra-Toohey L, Campeau T, Dagnone E, Lyver M, Ontario Prehospital Advanced Life Support Study Group Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351:647–656. doi: 10.1056/NEJMoa040325. - DOI - PubMed
-
- Nichol G, Thomas E, Callaway CW, Hedges J, Powell JL, Aufderheide TP, Rea T, Lowe R, Brown T, Dreyer J, Davis D, Idris A, Stiell I, Resuscitation Outcomes Consortium Investigators Regional variation in out-of-hospital cardiac arrest incidence and outcome. JAMA. 2008;300:1423–1431. doi: 10.1001/jama.300.12.1423. - DOI - PMC - PubMed
-
- Nolan JP, Soar J, Zideman DA, Biarent D, Bossaert LL, Deakin C, Koster RW, Wyllie J, Böttiger B, ERC Guidelines Writing Group European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation. 2010;81:1219–1276. doi: 10.1016/j.resuscitation.2010.08.021. - DOI - PubMed
-
- Lemiale V, Dumas F, Mongardon N, Giovanetti O, Charpentier J, Chiche JD, Carli P, Mira JP, Nolan J, Cariou A. Intensive care unit mortality after cardiac arrest: the relative contribution of shock and brain injury in a large cohort. Intensive Care Med. 2013;39:1972–1980. doi: 10.1007/s00134-013-3043-4. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
