

Metabolic signatures of adiposity in young adults: Mendelian randomization analysis and effects of weight change
- PMID: 25490400
- PMCID: PMC4260795
- DOI: 10.1371/journal.pmed.1001765
Metabolic signatures of adiposity in young adults: Mendelian randomization analysis and effects of weight change
Abstract
Background: Increased adiposity is linked with higher risk for cardiometabolic diseases. We aimed to determine to what extent elevated body mass index (BMI) within the normal weight range has causal effects on the detailed systemic metabolite profile in early adulthood.
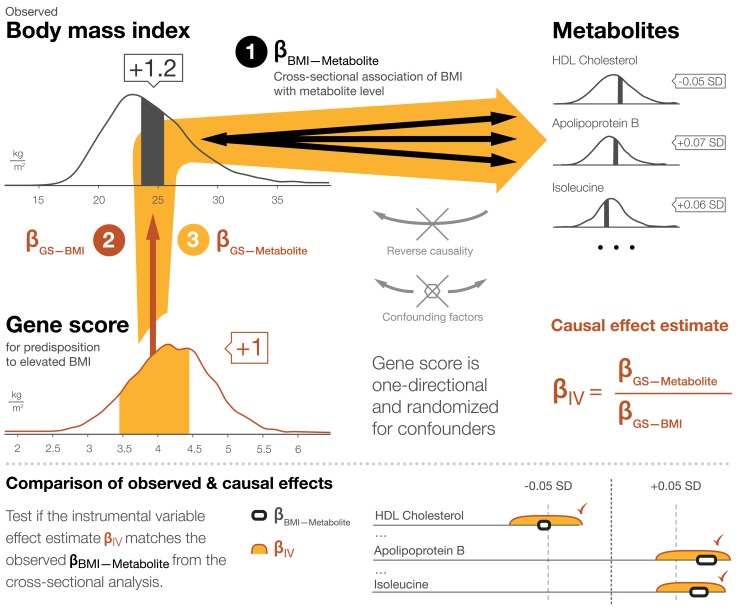
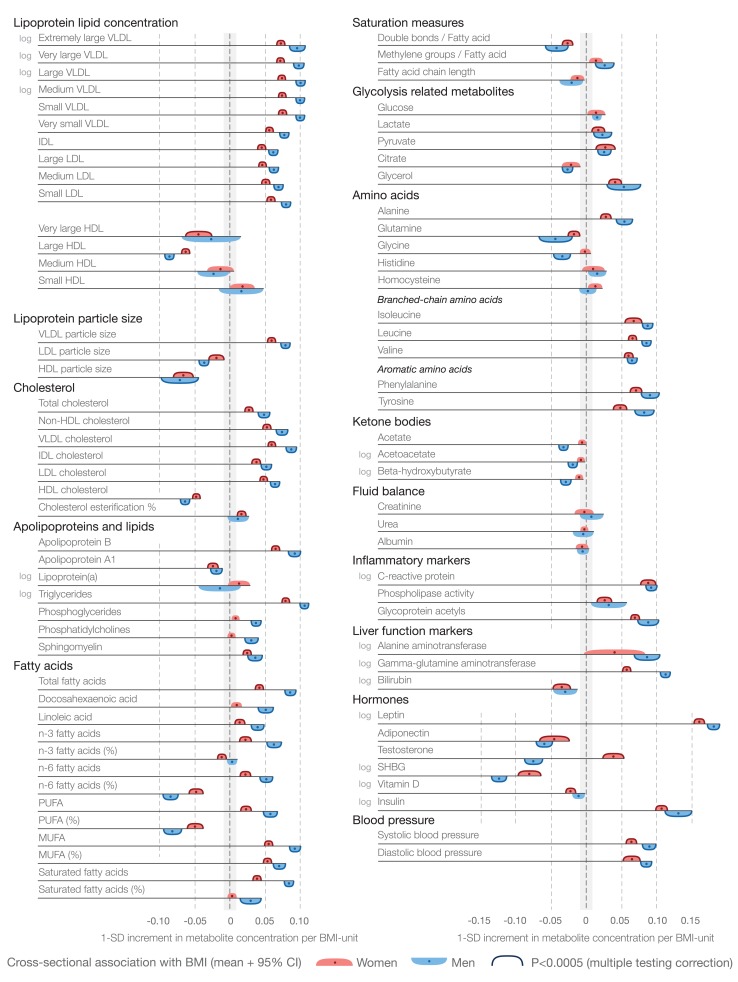
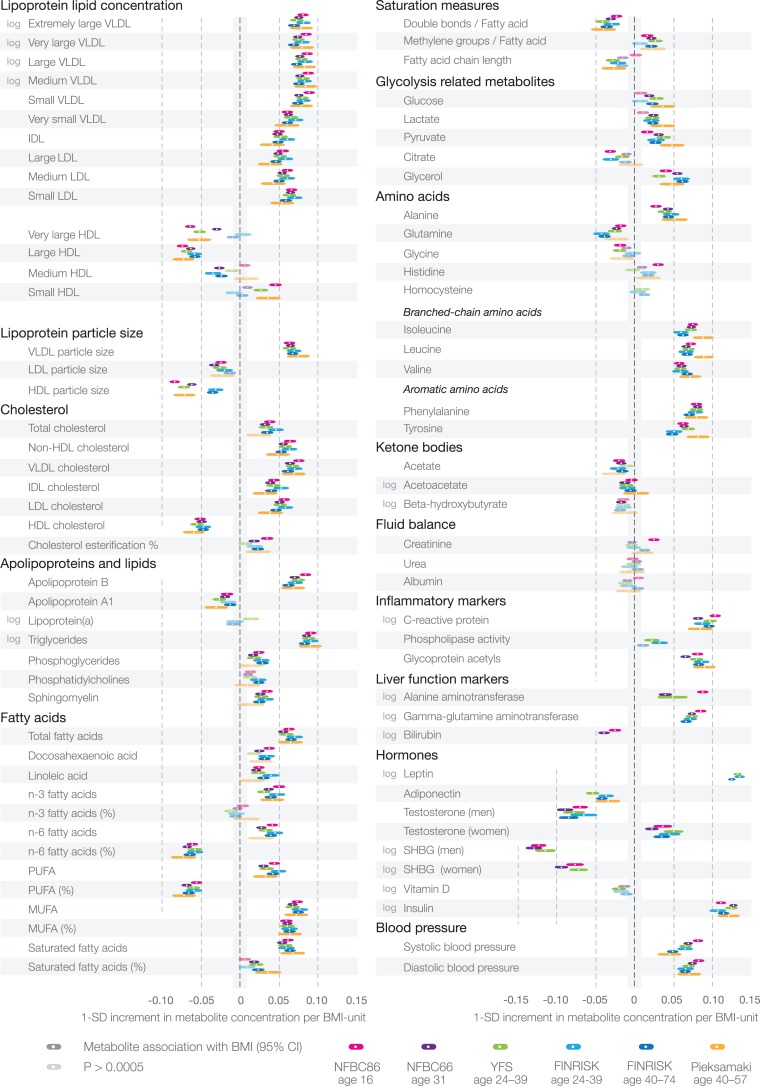
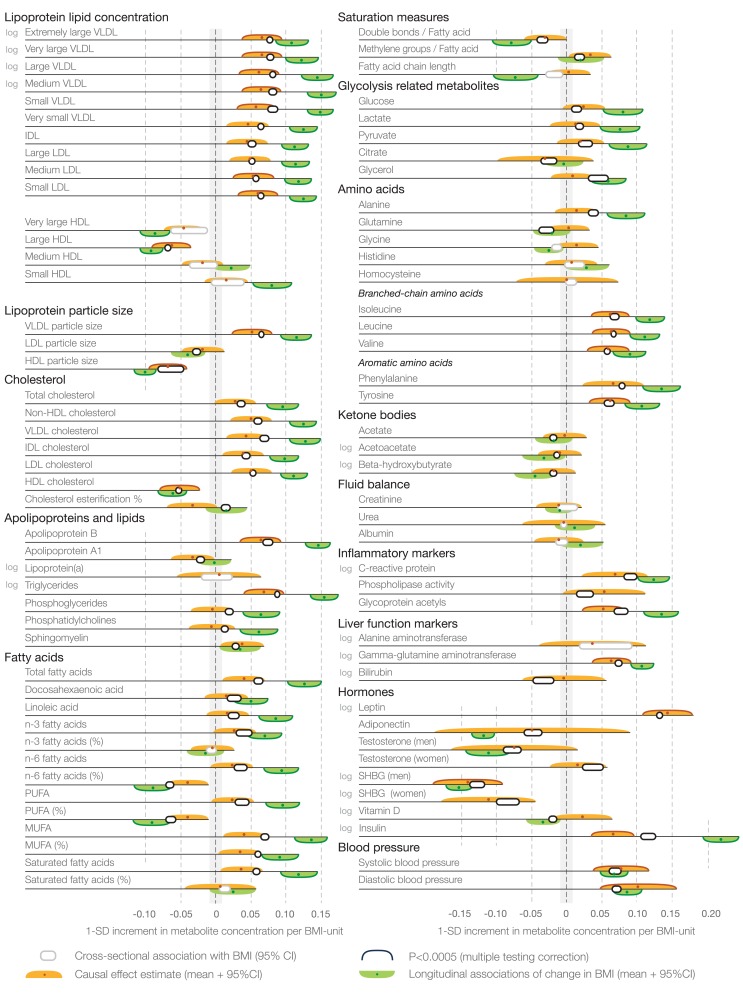
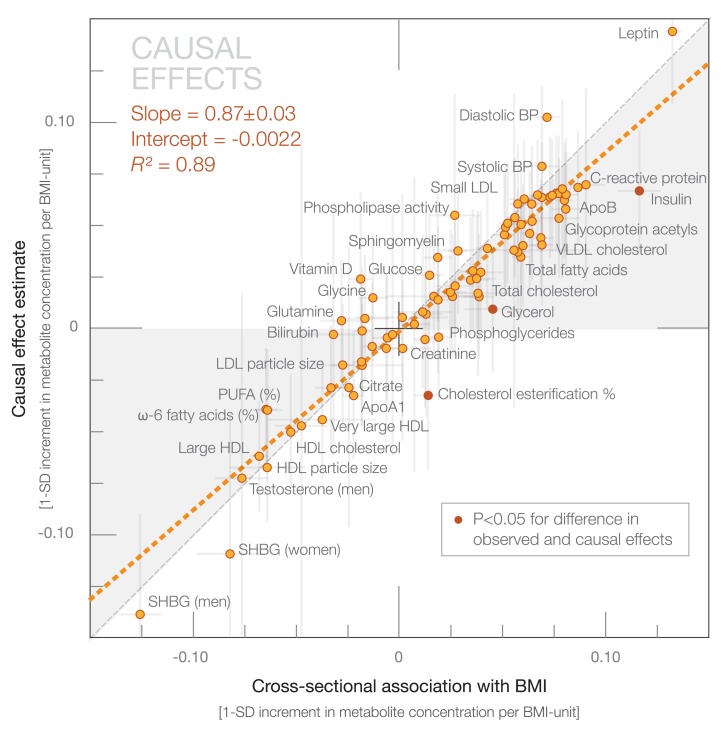
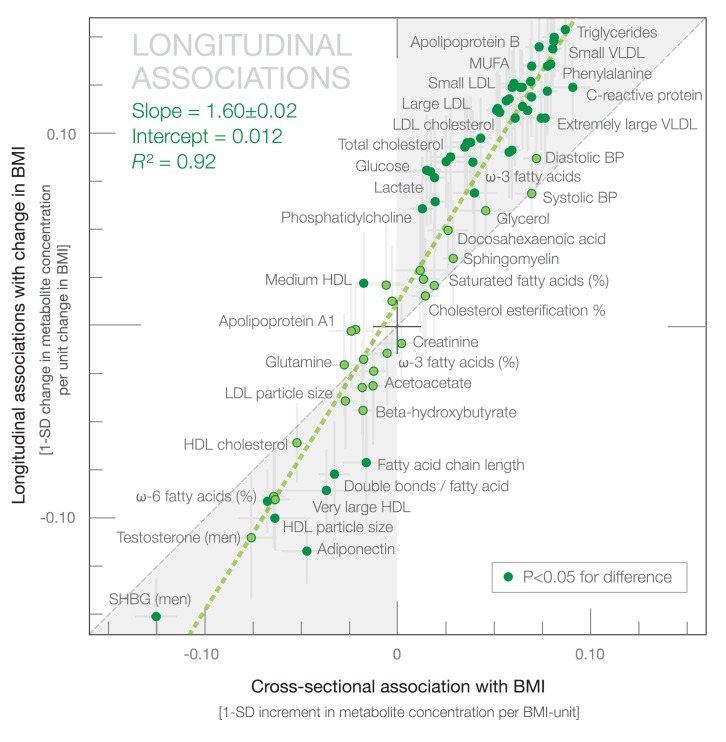
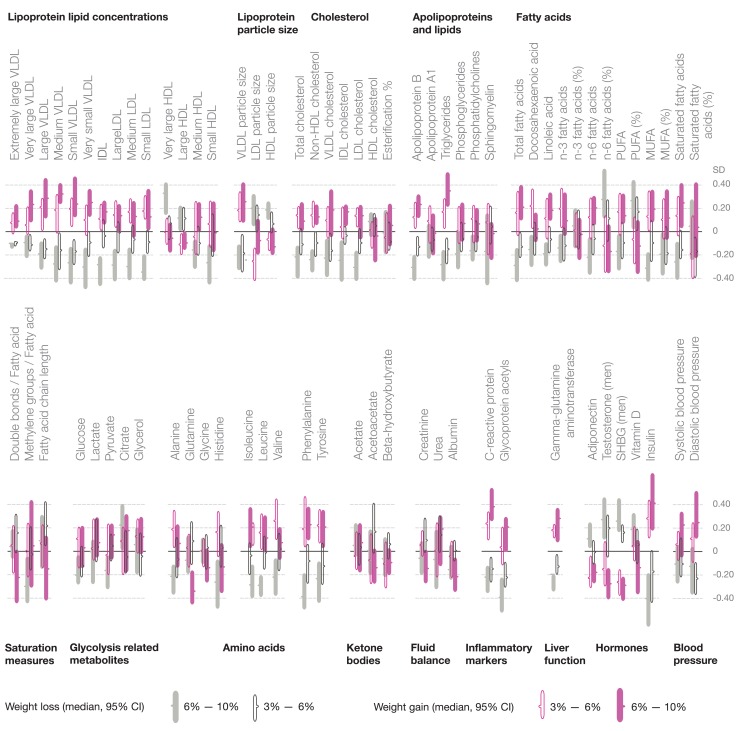
Methods and findings: We used Mendelian randomization to estimate causal effects of BMI on 82 metabolic measures in 12,664 adolescents and young adults from four population-based cohorts in Finland (mean age 26 y, range 16-39 y; 51% women; mean ± standard deviation BMI 24 ± 4 kg/m(2)). Circulating metabolites were quantified by high-throughput nuclear magnetic resonance metabolomics and biochemical assays. In cross-sectional analyses, elevated BMI was adversely associated with cardiometabolic risk markers throughout the systemic metabolite profile, including lipoprotein subclasses, fatty acid composition, amino acids, inflammatory markers, and various hormones (p<0.0005 for 68 measures). Metabolite associations with BMI were generally stronger for men than for women (median 136%, interquartile range 125%-183%). A gene score for predisposition to elevated BMI, composed of 32 established genetic correlates, was used as the instrument to assess causality. Causal effects of elevated BMI closely matched observational estimates (correspondence 87% ± 3%; R(2)= 0.89), suggesting causative influences of adiposity on the levels of numerous metabolites (p<0.0005 for 24 measures), including lipoprotein lipid subclasses and particle size, branched-chain and aromatic amino acids, and inflammation-related glycoprotein acetyls. Causal analyses of certain metabolites and potential sex differences warrant stronger statistical power. Metabolite changes associated with change in BMI during 6 y of follow-up were examined for 1,488 individuals. Change in BMI was accompanied by widespread metabolite changes, which had an association pattern similar to that of the cross-sectional observations, yet with greater metabolic effects (correspondence 160% ± 2%; R(2) = 0.92).
Conclusions: Mendelian randomization indicates causal adverse effects of increased adiposity with multiple cardiometabolic risk markers across the metabolite profile in adolescents and young adults within the non-obese weight range. Consistent with the causal influences of adiposity, weight changes were paralleled by extensive metabolic changes, suggesting a broadly modifiable systemic metabolite profile in early adulthood. Please see later in the article for the Editors' Summary.
Conflict of interest statement
PW, AJK, PS, and MAK are shareholders of Brainshake Ltd, a startup company offering NMR-based metabolite profiling. SB has received research funding from Abbott, Abbott Diagnostics, Bayer, Boehringer Ingelheim, SIEMENS, and Thermo Fisher. SB has received honoraria for lectures from Abbott, Abbott Diagnostics, Astra Zeneca, Bayer, Boehringer Ingelheim, Medtronic, Pfizer, Roche, SIEMENS Diagnostics, SIEMENS, Thermo Fisher, and as member of Advisory Boards and for consulting for Boehringer Ingelheim, Bayer, Novartis, Roche, and Thermo Fisher. GDS is a member of the Editorial Board of
Figures
References
-
- Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration (BMI Mediated Effects) (2014) Lu Y, Hajifathalian K, Ezzati M, Woodward M, et al. (2014) Metabolic mediators of the effects of body-mass index, overweight, and obesity on coronary heart disease and stroke: a pooled analysis of 97 prospective cohorts with 1.8 million participants. Lancet 383: 970–983. - PMC - PubMed
-
- Lewis CE, McTigue KM, Burke LE, Poirier P, Eckel RH, et al. (2009) Mortality, health outcomes, and body mass index in the overweight range. Circulation 119: 3263–3271. - PubMed
-
- Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, et al. (2014) 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society. Circulation 129 25 Suppl 2: S102–S138. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
