

Tooth-borne vs bone-borne rapid maxillary expanders in late adolescence
- PMID: 25490552
- PMCID: PMC8631879
- DOI: 10.2319/030514-156.1
Tooth-borne vs bone-borne rapid maxillary expanders in late adolescence
Abstract
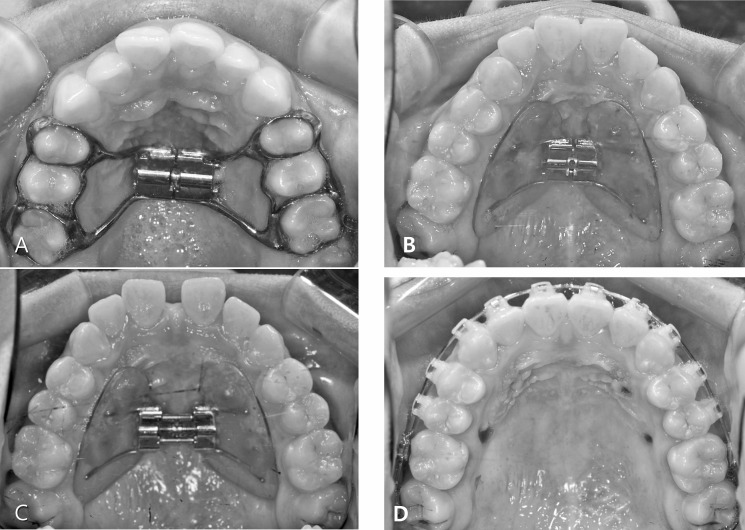
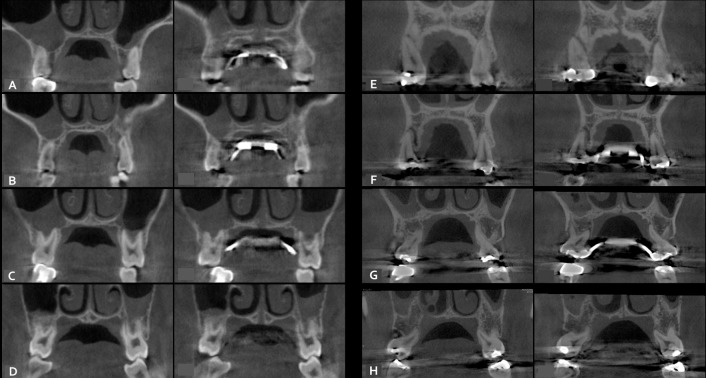
Objective: To evaluate the immediate effects of rapid maxillary expansion (RME) on the transverse skeletal and dentoalveolar changes with bone-borne (C-expander) and tooth-borne type expanders using cone-beam computed tomography (CBCT) in late adolescents.
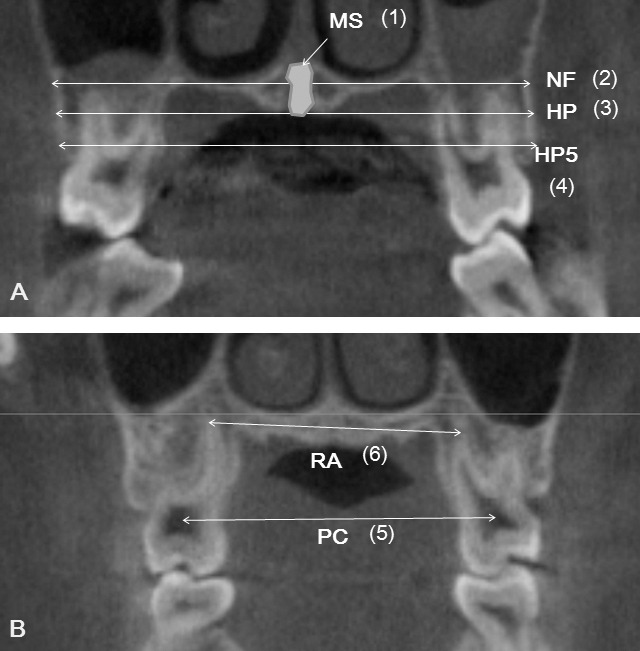
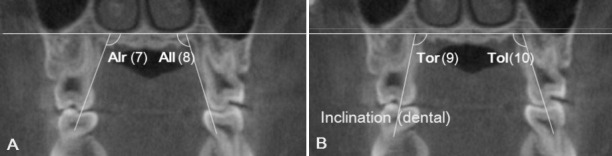
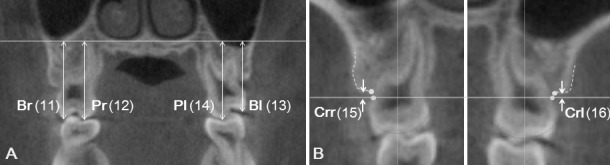
Materials and methods: A sample of 28 female late-adolescent patients was divided into two groups according to the type of expander: bone-borne (C-expander, n = 15, age = 18.1 ± 4.4 years) and tooth-borne (hyrax, bands on premolars and molars, n = 13, age = 17.4 ± 3.4 years). CBCT scans were taken at 0.2-mm voxel size before treatment (T1) and 3 months after RME (T2). Transverse skeletal and dental expansion, alveolar inclination, tooth axis, vertical height of tooth, and buccal dehiscence were evaluated on maxillary premolars and molars. Paired t-test, independent t-test, one-way analysis of variance, and Scheffé post hoc analysis were performed.
Results: The C-expander group produced greater skeletal expansion, except in the region of the first premolar (P < .05 or < .01), which showed slight buccal tipping of the alveolar bone. The Hyrax group had more buccal tipping of the alveolar bone and the tooth axes, except in the region of the second molar (P < .05 or < .01 or < .001). Dental expansion at the apex level was similar in the banded teeth (the first premolar and the first molar). Vertical height changes were apparent on the second premolar in the hyrax group (P < .05 or < .01). Significant buccal dehiscence occurred at the first premolar in the hyrax group (P < .01 or < .001). There were no significant differences between tooth types for any variables in the C-expander group.
Conclusions: For patients in late adolescence, bone-borne expanders produced greater orthopedic effects and fewer dentoalveolar side effects compared to the hyrax expanders.
Keywords: Alveolar bone; Bone-borne expander; C-implant; Cone-beam computed tomogram; Hyrax expander; Rapid maxillary expansion.
Figures

References
-
- Bishara SE, Jakobsen JR, Treder J, Nowak A. Arch width changes from 6 weeks to 45 years of age. Am J Orthod Dentofacial Orthop. 1997;111:401–409. - PubMed
-
- Baccetti T, Franchi L, Cameron CG, McNamara JA., Jr Treatment timing for rapid maxillary expansion. Angle Orthod. 2001;71:343–350. - PubMed
-
- Erverdi N, Okar I, Kucukkeles N, Arbak S. A comparison of two different rapid palatal expansion techniques from the point of root resorption. Am J Orthod Dentofacial Orthop. 1994;106:47–51. - PubMed
-
- Weissheimer A, de Menezes LM, Mezomo M, Dias DM, de Lima EM, Rizzatto SM. Immediate effects of rapid maxillary expansion with Haas-type and hyrax-type expanders: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2011;140:366–376. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
