

Increasing the use of second-line therapy is a cost-effective approach to prevent the spread of drug-resistant HIV: a mathematical modelling study
- PMID: 25491351
- PMCID: PMC4260459
- DOI: 10.7448/IAS.17.1.19164
Increasing the use of second-line therapy is a cost-effective approach to prevent the spread of drug-resistant HIV: a mathematical modelling study
Abstract
Introduction: Earlier antiretroviral therapy (ART) initiation reduces HIV-1 incidence. This benefit may be offset by increased transmitted drug resistance (TDR), which could limit future HIV treatment options. We analyze the epidemiological impact and cost-effectiveness of strategies to reduce TDR.
Methods: We develop a deterministic mathematical model representing Kampala, Uganda, to predict the prevalence of TDR over a 10-year period. We then compare the impact on TDR and cost-effectiveness of: (1) introduction of pre-therapy genotyping; (2) doubling use of second-line treatment to 80% (50-90%) of patients with confirmed virological failure on first-line ART; and (3) increasing viral load monitoring from yearly to twice yearly. An intervention can be considered cost-effective if it costs less than three times the gross domestic product per capita per quality adjusted life year (QALY) gained, or less than $3420 in Uganda.
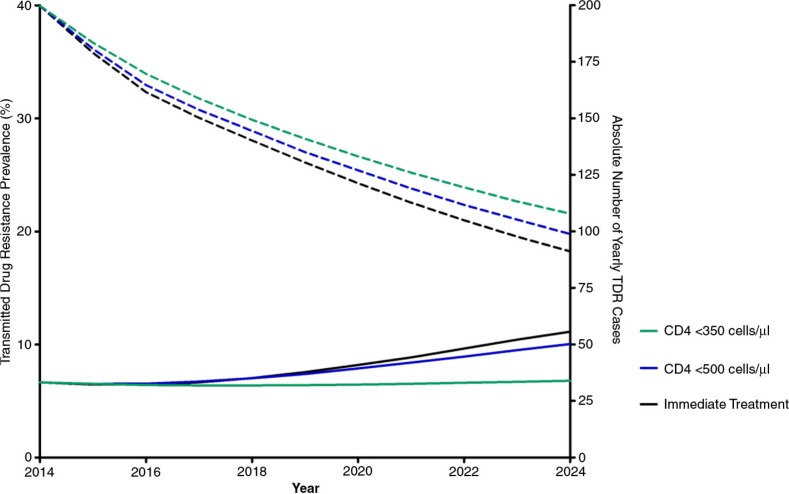
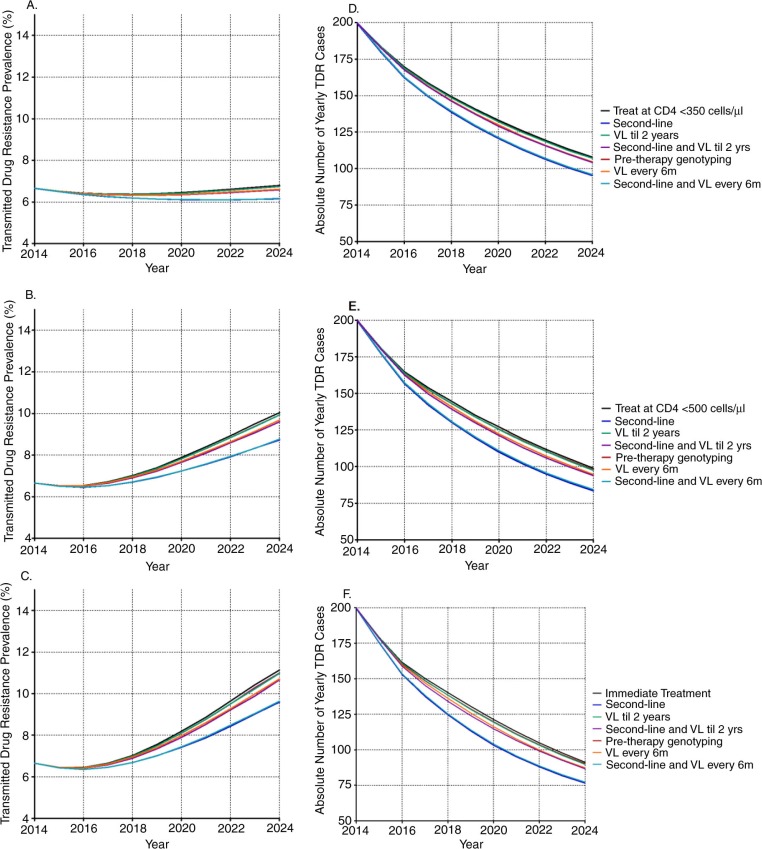
Results: The prevalence of TDR is predicted to rise from 6.7% (interquartile range [IQR] 6.2-7.2%) in 2014, to 6.8% (IQR 6.1-7.6%), 10.0% (IQR 8.9-11.5%) and 11.1% (IQR 9.7-13.0%) in 2024 if treatment is initiated at a CD4 <350, <500, or immediately, respectively. The absolute number of TDR cases is predicted to decrease 4.4-8.1% when treating earlier compared to treating at CD4 <350 due to the preventative effects of earlier treatment. Most cases of TDR can be averted by increasing second-line treatment (additional 7.1-10.2% reduction), followed by increased viral load monitoring (<2.7%) and pre-therapy genotyping (<1.0%). Only increasing second-line treatment is cost-effective, ranging from $1612 to $2234 (IQR $450-dominated) per QALY gained.
Conclusions: While earlier treatment initiation will result in a predicted increase in the proportion of patients infected with drug-resistant HIV, the absolute numbers of patients infected with drug-resistant HIV is predicted to decrease. Increasing use of second-line treatment to all patients with confirmed failure on first-line therapy is a cost-effective approach to reduce TDR. Improving access to second-line ART is therefore a major priority.
Keywords: antiretroviral therapy; cost-effectiveness; drug resistance; pre-therapy genotyping; second-line treatment; viral load monitoring.
Figures
References
-
- UNAIDS. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2013. Global report: UNAIDS report on the global AIDS epidemic 2013.
-
- Eaton JW, Menzies NA, Stover J, Cambiano V, Chindelevitch L, Cori A, et al. How should HIV programmes respond to evidence for the benefit of earlier treatment initiation? A combined analysis of twelve mathematical models. Lancet Global Health. 2014;2:e23–34. - PubMed
-
- WHO. Geneva: World Health Organization; 2013. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach. - PubMed
-
- Nichols BE, Sigaloff KC, Kityo C, Mandaliya K, Hamers RL, Bertagnolio S, et al. Averted HIV infections due to expanded antiretroviral treatment eligibility offsets risk of transmitted drug resistance: a modeling study. AIDS. 2014;28:73–83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
