

Effect of L-type calcium channel blocker (amlodipine) on myocardial iron deposition in patients with thalassaemia with moderate-to-severe myocardial iron deposition: protocol for a randomised, controlled trial
- PMID: 25492271
- PMCID: PMC4265146
- DOI: 10.1136/bmjopen-2014-005360
Effect of L-type calcium channel blocker (amlodipine) on myocardial iron deposition in patients with thalassaemia with moderate-to-severe myocardial iron deposition: protocol for a randomised, controlled trial
Abstract
Introduction: Sideroblastic cardiomyopathy secondary to repeated blood transfusions is a feared complication in thalassaemia. Control of myocardial iron is thus becoming the cornerstone of thalassaemia management. Recent evidence suggests a role for L-type Ca(2+) channels in mediating iron uptake by the heart. Blocking the cellular iron uptake through these channels may add to the benefit of therapy to standard chelation in reducing myocardial iron. We aim to determine the efficacy of amlodipine (a calcium channel blocker) as an adjunct to standard aggressive chelation in retarding myocardial iron deposition in thalassaemics with or without cardiomyopathy.
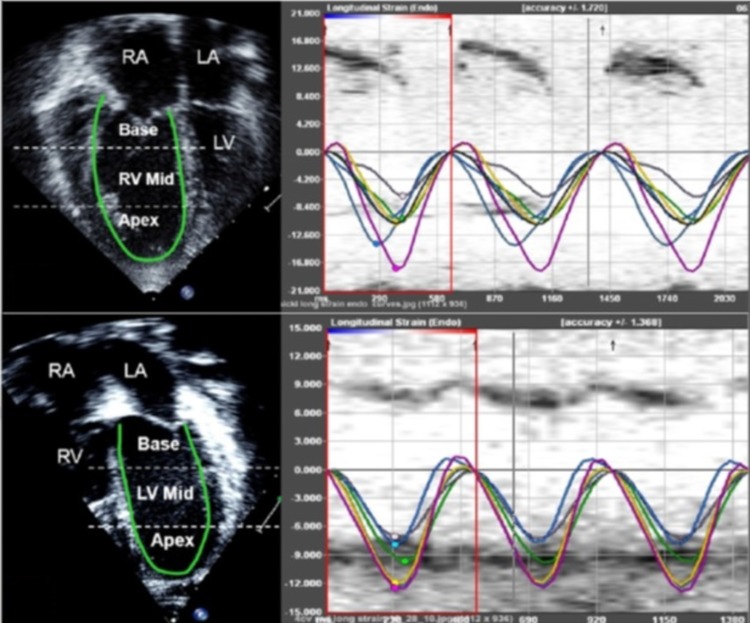
Outcomes: The primary outcome is to compare the efficacy of amlodipine+chelation (intervention) versus standard chelation (control) in retarding myocardial iron deposition. Secondary outcomes include the effect of amlodipine therapy on systolic and diastolic function, strain and strain rate and liver iron content.
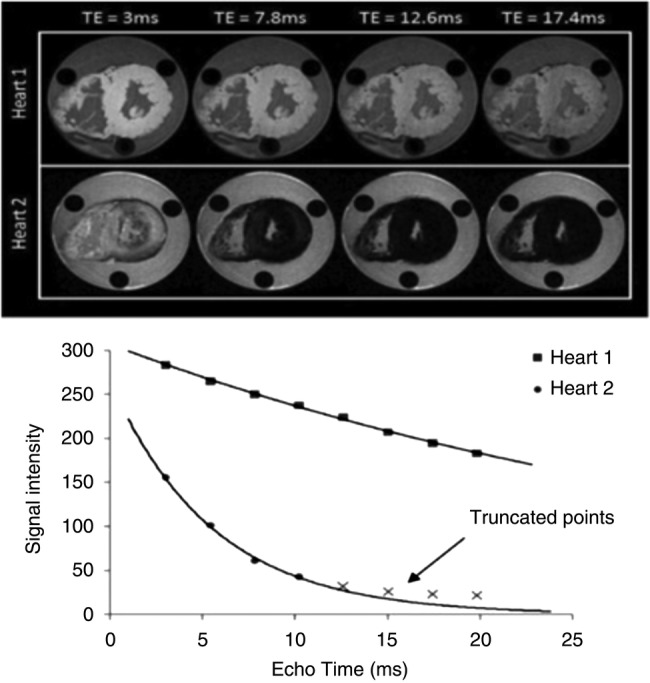
Methods and analysis: This is a single-centre, parallel-group, prospective randomised control trial. Twenty patients will be randomised in a 1:1 allocation ratio into the intervention and control arms. In addition to conventional echocardiography, MRI T2* values for assessment of cardiac and liver iron load will be obtained at baseline and at 6 and 12 months. Cardiac T2* will be reported as the geometric mean and per cent coefficient of variation, and an increase in cardiac T2* values from baseline will be used as an end point to compare the efficacy of therapy. A p Value of <0.05 will be considered significant.
Study setting: Department of Pediatric and Child Health, Aga Khan University Hospital, Karachi, Pakistan.
Ethics and dissemination: This study has been approved by the Ethics Review Committee and Clinical Trials Unit at The Aga Khan University with respect to scientific content and compliance with applicable research and human subjects regulations. Findings will be reported through scientific publications and research conferences and project summary papers for participants.
Trial registration number: ClinicalTrials.Gov. Registration no: NCT02065492.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Khateeb B, Moatter T, Shaghil AM et al. . Genetic diversity of beta-thalassemia mutations in Pakistani population. J Pak Med Assoc 2000;50:293–6. - PubMed
-
- Rahman M, Lodhi Y. Prospects and future of conservative management of beta thalassemia major in a developing country. Pak J Med Sci 2004;20:105–12.
-
- Arif F, Fayyaz J, Hamid A. Awareness among parents of children with thalassemia major. J Pak Med Assoc 2008;58:621–4. - PubMed
-
- Yang T, Brittenham GM, Dong WQ et al. . Deferoxamine prevents cardiac hypertrophy and failure in the gerbil model of iron-induced cardiomyopathy. J Lab Clin Med 2003;142:332–40. - PubMed
-
- Yang T, Dong WQ, Kuryshev YA et al. . Bimodal cardiac dysfunction in an animal model of iron overload. J Lab Clin Med 2002;140:263–71. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous