Transrectal ultrasonography of anorectal diseases: advantages and disadvantages
- PMID: 25492891
- PMCID: PMC4282231
- DOI: 10.14366/usg.14051
Transrectal ultrasonography of anorectal diseases: advantages and disadvantages
Abstract
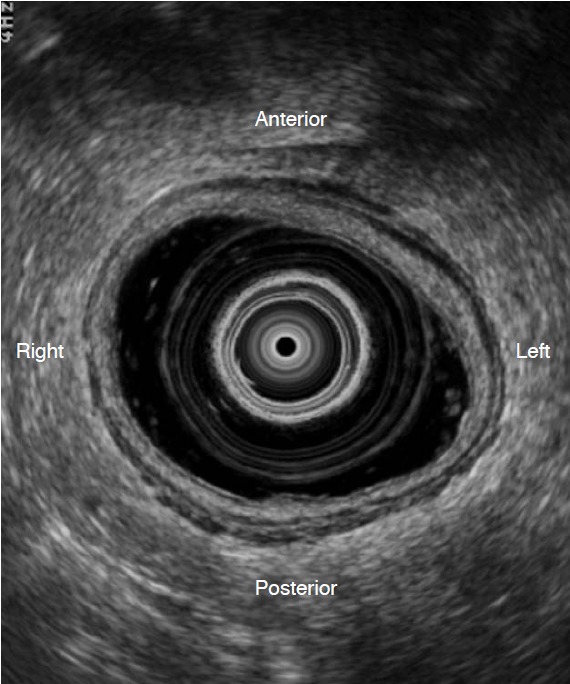
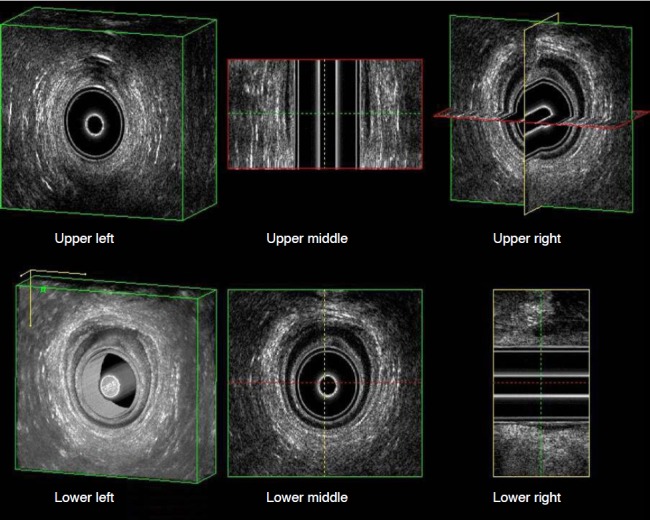
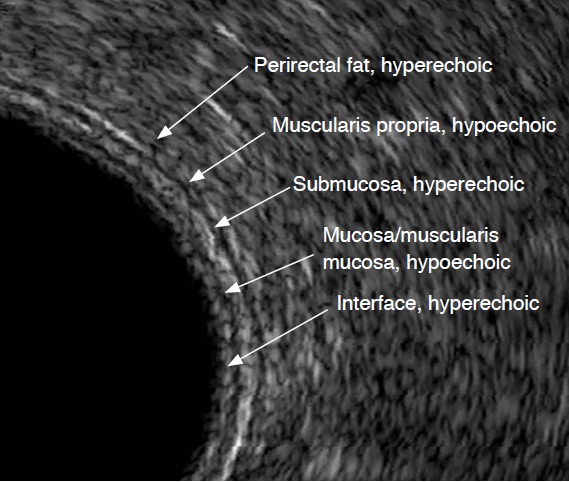
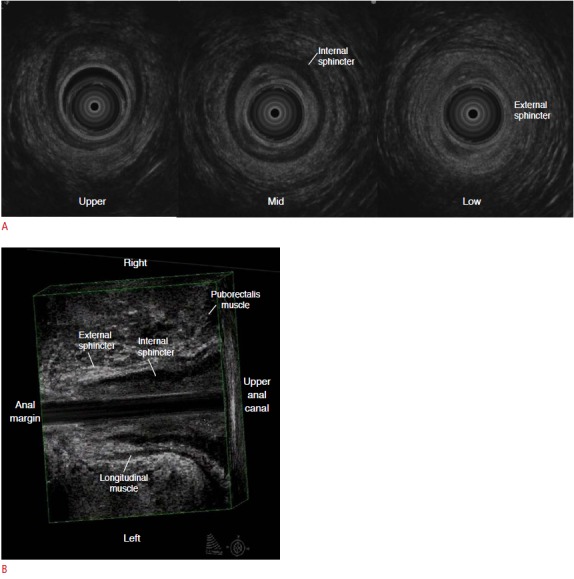
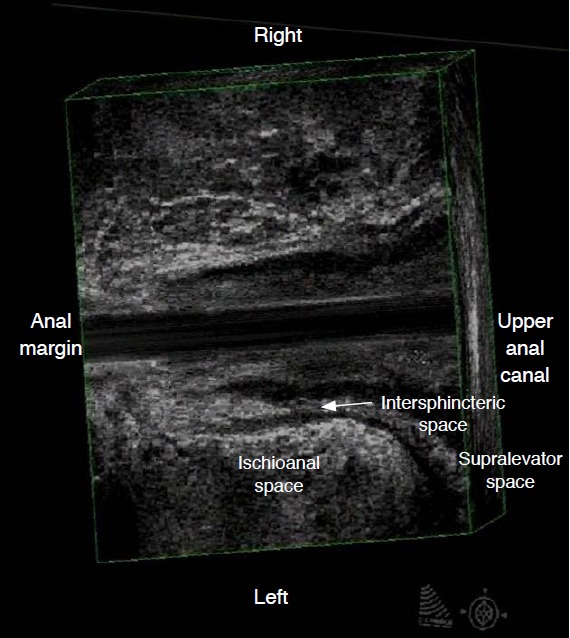
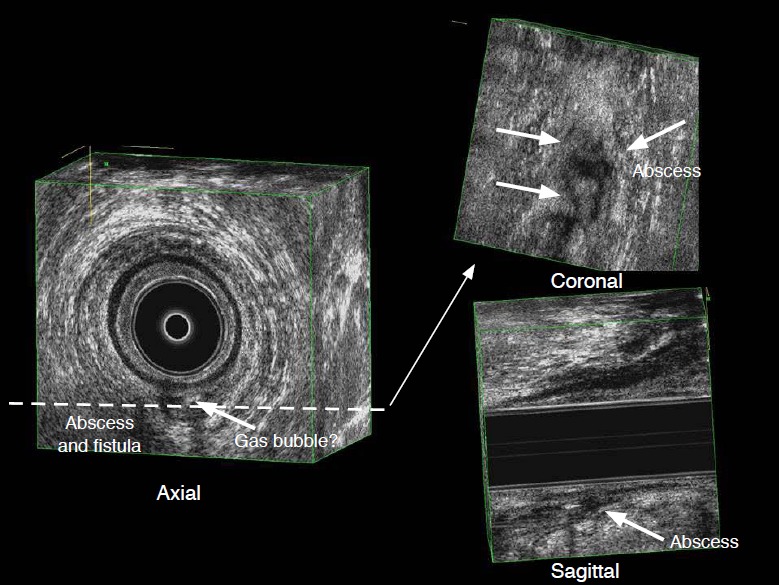
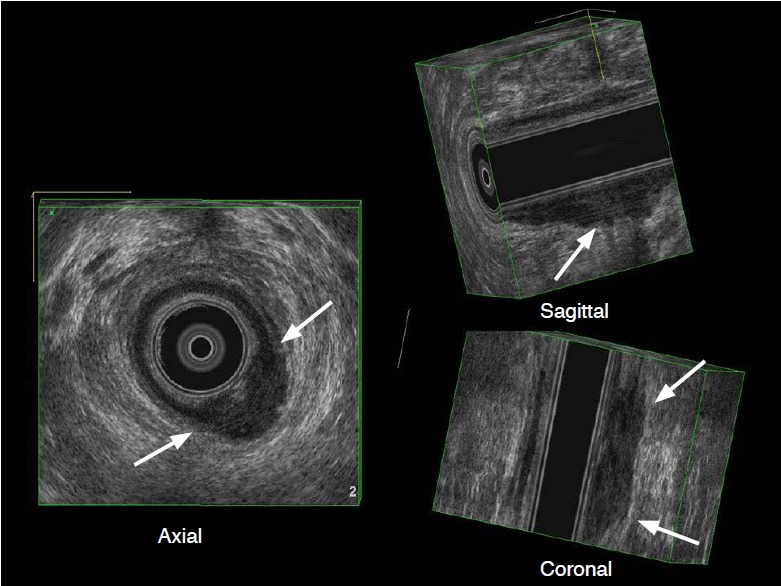
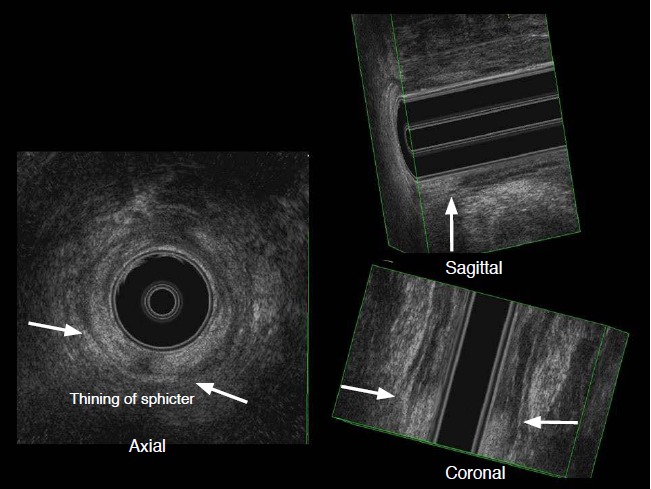
Transrectal ultrasonography (TRUS) has been widely accepted as a popular imaging modality for evaluating the lower rectum, anal sphincters, and pelvic floor in patients with various anorectal diseases. It provides excellent visualization of the layers of the rectal wall and of the anatomy of the anal canal. TRUS is an accurate tool for the staging of primary rectal cancer, especially for early stages. Although magnetic resonance imaging is a modality complementary to TRUS with advantages for evaluating the mesorectum, external sphincter, and deep pelvic inflammation, three-dimensional ultrasonography improves the detection and characterization of perianal fistulas and therefore plays a crucial role in optimal treatment planning. The operator should be familiar with the anatomy of the rectum and pelvic structures relevant to the preoperative evaluation of rectal cancer and other anal canal diseases, and should have technical proficiency in the use of TRUS combined with an awareness of its limitations compared to magnetic resonance imaging.
Keywords: Anal canal; Fistula; Rectal neoplasms; Ultrasonography.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
[Anorectal functional study. The state of the art].Minerva Chir. 1994 Dec;49(12):1187-93. Minerva Chir. 1994. PMID: 7746437 Review. Italian.
-
Endosonographic imaging of anorectal diseases.J Ultrasound Med. 2006 Jan;25(1):57-73. doi: 10.7863/jum.2006.25.1.57. J Ultrasound Med. 2006. PMID: 16371556 Review.
-
Endoanorectal ultrasonography.Ultrasound Q. 2011 Jun;27(2):87-104. doi: 10.1097/RUQ.0b013e31821c7f21. Ultrasound Q. 2011. PMID: 21606791 Review.
-
Comparative study of transrectal ultrasonography, pelvic computerized tomography, and magnetic resonance imaging in preoperative staging of rectal cancer.Dis Colon Rectum. 1999 Jun;42(6):770-5. doi: 10.1007/BF02236933. Dis Colon Rectum. 1999. PMID: 10378601
-
Endosonography in anorectal disease: an overview.Scand J Gastroenterol Suppl. 2006;(243):165-74. doi: 10.1080/00365520600664292. Scand J Gastroenterol Suppl. 2006. PMID: 16782637 Review.
Cited by
-
Hepatic and Intra-abdominal Tuberculosis: 2016 Update.Curr Infect Dis Rep. 2016 Dec;18(12):45. doi: 10.1007/s11908-016-0546-5. Curr Infect Dis Rep. 2016. PMID: 27796776 Review.
-
The accuracy of endorectal ultrasonography in rectal cancer staging.Clujul Med. 2015;88(3):348-56. doi: 10.15386/cjmed-481. Epub 2015 Jul 1. Clujul Med. 2015. PMID: 26609269 Free PMC article.
-
Transrectal Ultra Sonography based evidence of Ksharasutra therapy for Fistula-in-ano - A case series.J Ayurveda Integr Med. 2017 Apr-Jun;8(2):113-121. doi: 10.1016/j.jaim.2017.01.013. Epub 2017 Jun 7. J Ayurveda Integr Med. 2017. PMID: 28600166 Free PMC article.
-
Utility of Endoanal Ultrasonography in Assessment of Primary and Recurrent Anal Fistulas and for Detection of Associated Anal Sphincter Defects.J Gastrointest Surg. 2017 Nov;21(11):1879-1887. doi: 10.1007/s11605-017-3574-z. Epub 2017 Sep 11. J Gastrointest Surg. 2017. PMID: 28895031
-
High-resolution direct magnetic resonance imaging fistulography with hydrogen peroxide for diagnosing anorectal fistula: A preliminary retrospective study.World J Radiol. 2025 Jan 28;17(1):101221. doi: 10.4329/wjr.v17.i1.101221. World J Radiol. 2025. PMID: 39876881 Free PMC article.
References
-
- Engin G. Endosonographic imaging of anorectal diseases. J Ultrasound Med. 2006;25:57–73. - PubMed
-
- Saranovic D, Barisic G, Krivokapic Z, Masulovic D, Djuric-Stefanovic A. Endoanal ultrasound evaluation of anorectal diseases and disorders: technique, indications, results and limitations. Eur J Radiol. 2007;61:480–489. - PubMed
-
- Saftoiu A, Gheonea DI. Tridimensional (3D) endoscopic ultrasound: a pictorial review. J Gastrointestin Liver Dis. 2009;18:501–505. - PubMed
-
- Samdani T, Garcia-Aguilar J. Imaging in rectal cancer: magnetic resonance imaging versus endorectal ultrasonography. Surg Oncol Clin N Am. 2014;23:59–77. - PubMed
-
- Cartana ET, Parvu D, Saftoiu A. Endoscopic ultrasound: current role and future perspectives in managing rectal cancer patients. J Gastrointestin Liver Dis. 2011;20:407–413. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources