

Overcoming endocrine resistance in metastatic breast cancer: Current evidence and future directions
- PMID: 25493235
- PMCID: PMC4259959
- DOI: 10.5306/wjco.v5.i5.990
Overcoming endocrine resistance in metastatic breast cancer: Current evidence and future directions
Abstract
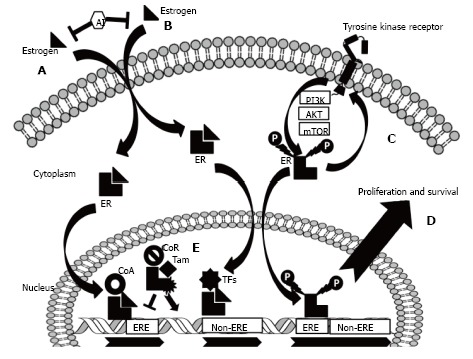
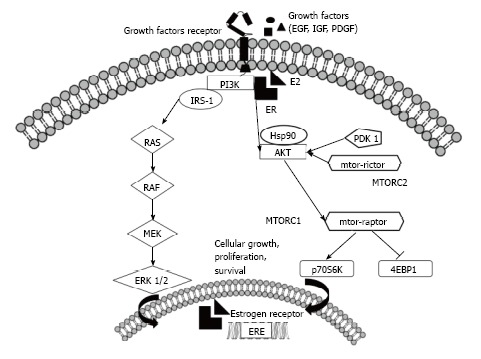
About 75% of all breast cancers are estrogen receptor (ER)-positive. They generally have a more favorable clinical behavior, prognosis, and pattern of recurrence, and endocrine therapy forms the backbone of treatment. Anti-estrogens (such as tamoxifen and fulvestrant) and aromatase inhibitors (such as anastrozole, letrozole, and exemestane) can effectively control the disease and induce tumor responses in a large proportion of patients. However, the majority of patients progress during endocrine therapy (acquired resistance) and a proportion of patients may fail to respond to initial therapy (de novo resistance). Endocrine resistance is therefore of clinical concern and there is great interest in strategies that delay or circumvent it. A deeper knowledge of the molecular mechanisms that drive endocrine resistance has recently led to development of new strategies that have the promise to effectively overcome it. Many resistance mechanisms have been described, and the crosstalk between ER and growth factor receptor signaling pathways seems to represent one of the most relevant. Compounds that are able to inhibit key elements of these pathways and restore endocrine sensitivity have been studied and more are currently under development. The aim of this review is to summarize the molecular pathophysiology of endocrine resistance in breast cancer and its impact on current clinical management.
Keywords: Endocrine resistance; Estrogen receptor; Everolimus; Mammalian target of rapamycin; PI3K inhibitors.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Winkfield KM, Harris JR. Effective local therapy and long-term survival in breast cancer. Oncology (Williston Park) 2009;23:669–675. - PubMed
-
- Cady B, Michaelson JS, Chung MA. The „tipping point“ for breast cancer mortality decline has resulted from size reductions due to mammographic screening. Ann Surg Oncol. 2011;18:903–906. - PubMed
-
- Lal P, Tan LK, Chen B. Correlation of HER-2 status with estrogen and progesterone receptors and histologic features in 3,655 invasive breast carcinomas. Am J Clin Pathol. 2005;123:541–546. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
