

Evaluation of treatment plans using various treatment techniques for the radiotherapy of cutaneous Kaposi's sarcoma developed on the skin of feet
- PMID: 25493522
- PMCID: PMC5711114
- DOI: 10.1120/jacmp.v15i6.4970
Evaluation of treatment plans using various treatment techniques for the radiotherapy of cutaneous Kaposi's sarcoma developed on the skin of feet
Abstract
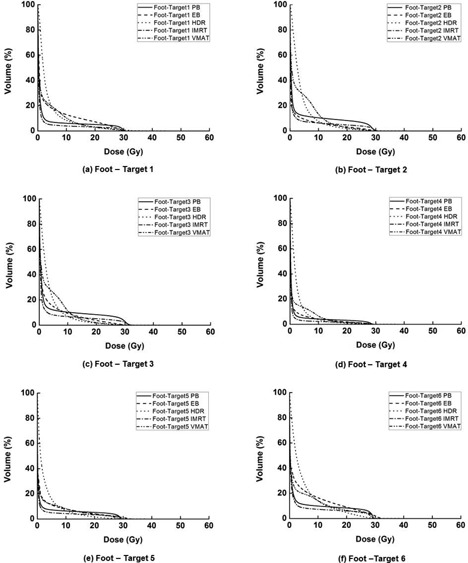
The purpose of this study was to investigate the plan qualities of various treatment modalities for the radiotherapy of cutaneous Kaposi's sarcoma developed on the skin of the foot. A total of six virtual targets were generated on the skin of the foot in CT images. Five types of treatment plans were generated using photon beams (PB), electron beams (EB), high-dose-rate (HDR) brachytherapy with a Freiburg flap applicator, intensity-modulated radiation therapy (IMRT), and volumetric- modulated arc therapy (VMAT) techniques. Plans for each of the six targets (single-target plans) and also for the combined target consisting of the six single targets combined (multitarget plans) were generated. Dose-volumetric analysis was performed for the targets and normal tissues. The averaged conformity index (CI) and homogeneity index (HI) values for each single target using PB, EB, HDR, IMRT, and VMAT techniques were 1.97, 2.39, 1.60, 4.60, and 0.80 and 1.05, 1.11, 1.52, 1.04, and 1.04, respectively. For the multitarget, the CI values were 3.99, 5.08, 1.38, 1.95, and 0.84, and the values of HI were 1.10, 1.36, 1.43, 1.06, and 1.04, respectively. The averaged mean doses to normal tissue were 2.5, 2.7, 3.6, 1.7, and 2.9 Gy for single-target plans, and 21.3, 14.6, 14.2, 14.3, and 13.0 Gy for the multitarget plans, respectively. The VMAT demonstrated dosimetric advantages and better treatment efficiency over other techniques for the radiotherapy of multifocal skin disease of the feet.
Figures








References
-
- Weshler Z, Loewinger E, Loewenthal E, Levinson R, Fucks Z. Megavoltage radiotherapy using water bolus in the treatment of Kaposi's sarcoma. Int J Radiat Oncol Biol Phys. 1986;12(11):2029–32. - PubMed
-
- Aldenhoven M, Barlo NP, Sanders CJ. Therapeutic strategies for epidemic Kaposi's sarcoma. Int J STD AIDS. 2006;17(9):571–78. - PubMed
-
- Stelzer KJ and Griffin TW. A randomized prospective trial of radiation therapy for AIDS‐associated Kaposi's sarcoma. Int J Radiat Oncol Biol Phys. 1993;27(5):1057–61. - PubMed
-
- Cohen L, Palmer PE, Nickson JJ. Treatment of Kaposi's sarcoma by radiation. Acta Unio Int Contra Cancrum. 1961;18:502–09. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
