

Very early administration of progesterone for acute traumatic brain injury
- PMID: 25493974
- PMCID: PMC4303469
- DOI: 10.1056/NEJMoa1404304
Very early administration of progesterone for acute traumatic brain injury
Abstract
Background: Traumatic brain injury (TBI) is a major cause of death and disability worldwide. Progesterone has been shown to improve neurologic outcome in multiple experimental models and two early-phase trials involving patients with TBI.
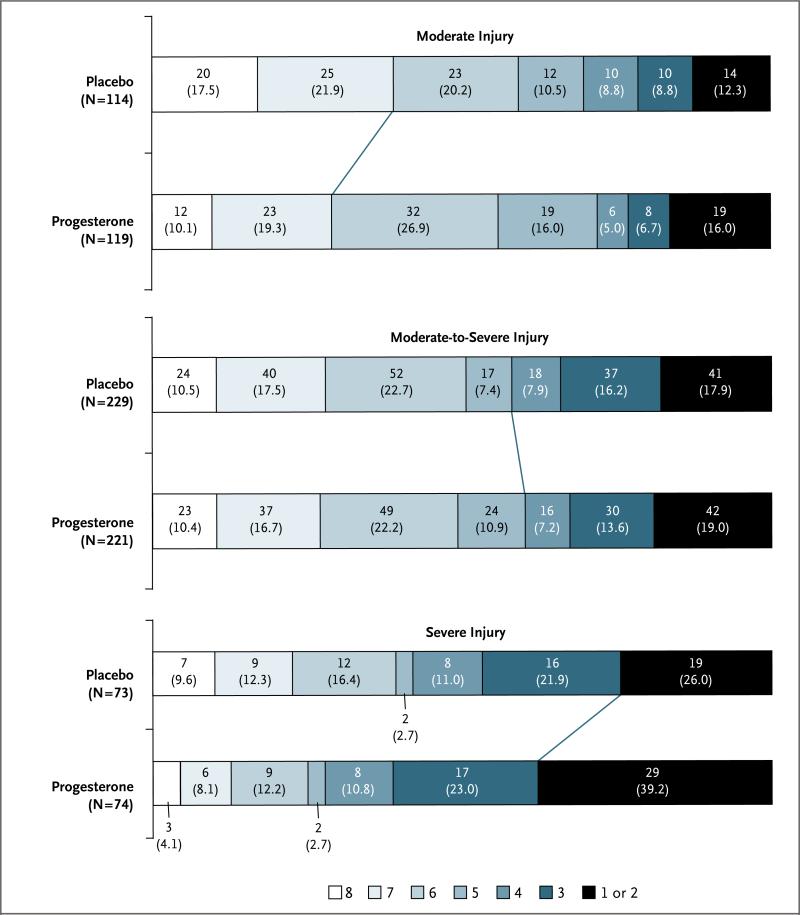
Methods: We conducted a double-blind, multicenter clinical trial in which patients with severe, moderate-to-severe, or moderate acute TBI (Glasgow Coma Scale score of 4 to 12, on a scale from 3 to 15, with lower scores indicating a lower level of consciousness) were randomly assigned to intravenous progesterone or placebo, with the study treatment initiated within 4 hours after injury and administered for a total of 96 hours. Efficacy was defined as an increase of 10 percentage points in the proportion of patients with a favorable outcome, as determined with the use of the stratified dichotomy of the Extended Glasgow Outcome Scale score at 6 months after injury. Secondary outcomes included mortality and the Disability Rating Scale score.
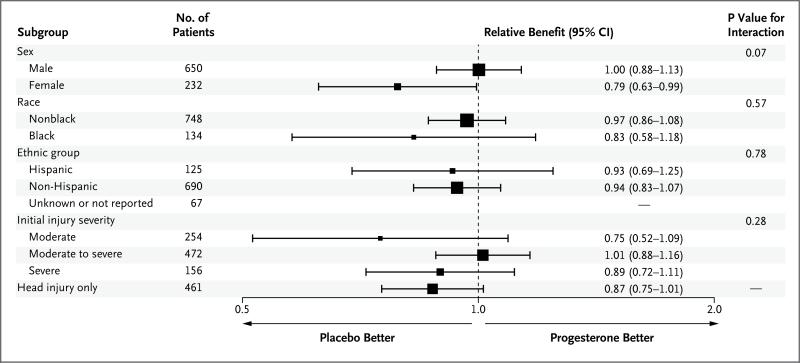
Results: A total of 882 of the planned sample of 1140 patients underwent randomization before the trial was stopped for futility with respect to the primary outcome. The study groups were similar with regard to baseline characteristics; the median age of the patients was 35 years, 73.7% were men, 15.2% were black, and the mean Injury Severity Score was 24.4 (on a scale from 0 to 75, with higher scores indicating greater severity). The most frequent mechanism of injury was a motor vehicle accident. There was no significant difference between the progesterone group and the placebo group in the proportion of patients with a favorable outcome (relative benefit of progesterone, 0.95; 95% confidence interval [CI], 0.85 to 1.06; P=0.35). Phlebitis or thrombophlebitis was more frequent in the progesterone group than in the placebo group (relative risk, 3.03; CI, 1.96 to 4.66). There were no significant differences in the other prespecified safety outcomes.
Conclusions: This clinical trial did not show a benefit of progesterone over placebo in the improvement of outcomes in patients with acute TBI. (Funded by the National Institute of Neurological Disorders and Stroke and others; PROTECT III ClinicalTrials.gov number, NCT00822900.).
Figures
Comment in
-
Progesterone for traumatic brain injury--resisting the sirens' song.N Engl J Med. 2014 Dec 25;371(26):2522-3. doi: 10.1056/NEJMe1412951. Epub 2014 Dec 10. N Engl J Med. 2014. PMID: 25493975 No abstract available.
-
Progesterone in traumatic brain injury.N Engl J Med. 2015 Apr 30;372(18):1766-7. doi: 10.1056/NEJMc1503138. N Engl J Med. 2015. PMID: 25923558 No abstract available.
-
Progesterone in traumatic brain injury.N Engl J Med. 2015 Apr 30;372(18):1765. doi: 10.1056/NEJMc1503138. N Engl J Med. 2015. PMID: 25923559 No abstract available.
-
Progesterone in traumatic brain injury.N Engl J Med. 2015 Apr 30;372(18):1765-6. doi: 10.1056/NEJMc1503138. N Engl J Med. 2015. PMID: 25923560 No abstract available.
References
-
- Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21:375–8. - PubMed
-
- Stein DG, Wright DW. Progesterone in the clinical treatment of acute traumatic brain injury. Expert Opin Investig Drugs. 2010;19:847–57. - PubMed
-
- Deutsch ER, Espinoza TR, Atif F, Woodall E, Kaylor J, Wright DW. Progesterone's role in neuroprotection, a review of the evidence. Brain Res. 2013;1530:82–105. - PubMed
-
- Wright DW, Kellermann AL, Hertz- berg VS, et al. ProTECT: a randomized clinical trial of progesterone for acute traumatic brain injury. Ann Emerg Med. 2007;49:391–402. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 NS062778/NS/NINDS NIH HHS/United States
- U10 NS059032/NS/NINDS NIH HHS/United States
- U10 NS058940/NS/NINDS NIH HHS/United States
- UL1TR000454/TR/NCATS NIH HHS/United States
- U01 NS059041/NS/NINDS NIH HHS/United States
- U10 NS080377/NS/NINDS NIH HHS/United States
- U01 NS056975/NS/NINDS NIH HHS/United States
- U10 NS080369/NS/NINDS NIH HHS/United States
- U01NS056975/NS/NINDS NIH HHS/United States
- 5U10NS059032/NS/NINDS NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- NS062778/NS/NINDS NIH HHS/United States
- U10 NS058960/NS/NINDS NIH HHS/United States
- U10 NS059012/NS/NINDS NIH HHS/United States
- UL1 TR001425/TR/NCATS NIH HHS/United States
- U10 NS058927/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical