

The Effect of the Diffusion of the Surgical Robot on the Hospital-level Utilization of Partial Nephrectomy
- PMID: 25494234
- PMCID: PMC4707949
- DOI: 10.1097/MLR.0000000000000259
The Effect of the Diffusion of the Surgical Robot on the Hospital-level Utilization of Partial Nephrectomy
Abstract
Introduction: The rapid diffusion of the surgical robot has been controversial because of the technology's high costs and its disputed marginal benefit. Some, however, have suggested that adoption of the robot may have improved care for patients with renal malignancy by facilitating partial nephrectomy, an underutilized, technically challenging procedure believed to be less morbid than radical nephrectomy. We sought to determine whether institutional acquisition of the robot was associated with increased utilization of partial nephrectomy.
Methods: We used all payer data from 7 states to identify 21,569 nephrectomies. These patient-level records were aggregated to the hospital-level then merged with the American Hospital Association Annual Survey and publicly available data on timing of robot acquisition. We used a multivariable difference-in-difference model to assess at the hospital-level whether robot acquisition was associated with an increase in the proportion of partial nephrectomy, adjusting for hospital nephrectomy volume, year of surgery, and several additional hospital-level factors.
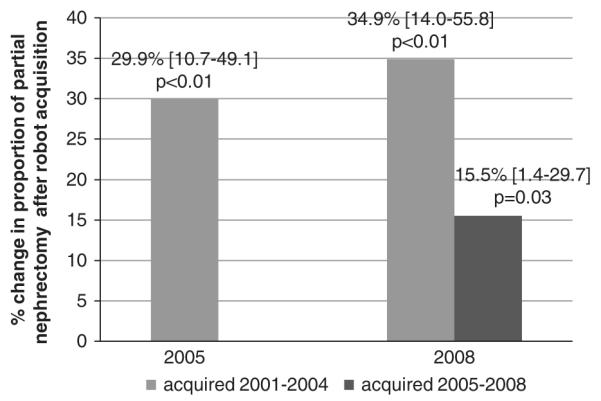
Results: In the multivariable-adjusted differences-in-differences model, hospitals acquiring a robot between 2001 and 2004 performed a greater proportion of partial nephrectomy in both 2005 (29.9% increase) and 2008 (34.9% increase). Hospitals acquiring a robot between 2005 and 2008 also demonstrated a greater proportion of partial nephrectomy in 2008 (15.5% increase). In addition, hospital nephrectomy volume and urban location were also significantly associated with increased proportion of partial nephrectomy.
Conclusions: Hospital acquisition of the surgical robot is associated with greater proportion of partial nephrectomy, an underutilized, guideline-encouraged procedure. This is one of the few studies to suggest robot acquisition is associated with improvement in quality of patient care.
Figures
References
-
- Kolata G. Results Unproven, Robotic Surgery Wins Converts. The New York Times. 2010 Feb 14; Health.
-
- Lotan Y, Cadeddu JA, Gettman MT. The new economics of radical prostatectomy: cost comparison of open, laparoscopic and robot assisted techniques. J Urol. 2004;172(4 pt 1):1431–1435. - PubMed
-
- Carreyrou J. [Accessed May 4, 2010];Surgical robot examined in injuries. Wall Street Journal. 2010 Available at: http://online.wsj.com/article/SB1000142405270230470310457517395214590752....
-
- Hu JC, Gu X, Lipsitz SR, et al. Comparative effectiveness of minimally invasive vs open radical prostatectomy. JAMA. 2009:1557–1564. - PubMed
-
- [Accessed May 2, 2013];da Vinci® Procedures. 2013 Available at: http://www.davincisurgery.com/da-vinci-surgery/da-vinci-procedures/
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
