

Review
doi: 10.1259/bjr.20140594.
Epub 2014 Dec 12.
Use of cardiac CT and calcium scoring for detecting coronary plaque: implications on prognosis and patient management
Affiliations
- PMID: 25494818
- PMCID: PMC4614250
- DOI: 10.1259/bjr.20140594
Item in Clipboard
Review
Use of cardiac CT and calcium scoring for detecting coronary plaque: implications on prognosis and patient management
Br J Radiol.
2015 Feb.
Abstract
Clinicians often use risk factor-based calculators to estimate an individual's risk of developing cardiovascular disease. Non-invasive cardiovascular imaging, particularly coronary artery calcium (CAC) scoring and coronary CT angiography (CTA), allows for direct visualization of coronary atherosclerosis. Among patients without prior coronary artery disease, studies examining CAC and coronary CTA have consistently shown that the presence, extent and severity of coronary atherosclerosis provide additional prognostic information for patients beyond risk factor-based scores alone. This review will highlight the basics of CAC scoring and coronary CTA and discuss their role in impacting patient prognosis and management.
Figures

Rate of cardiovascular death or myocardial infarction according to the presence, severity and extent of coronary artery disease (CAD). There is a significant difference (p < 0.01) in rates for all comparisons except non-obstructive CAD with segment involvement score >4 and obstructive CAD with segment involvement score (SIS) ≤4. Reproduced from Bittencourt et al with permission from Lippincott Williams and Wilkins/Wolters Kluwer Health. pt, patient.
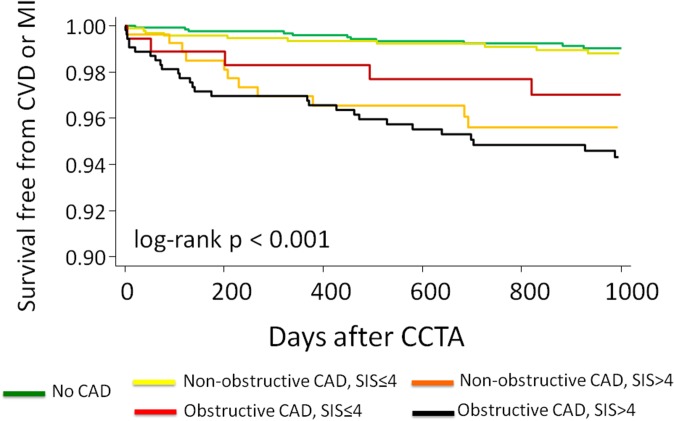
Survival free from cardiovascular death or myocardial infarction according to the presence, severity and extent of coronary artery disease. CAD, coronary artery disease; CCTA, coronary CT angiography; CVD, cardiovascular death; MI, myocardial infarction; SIS, segment involvement score. Reproduced from Bittencourt et al with permission from Lippincott Williams and Wilkins/Wolters Kluwer Health.
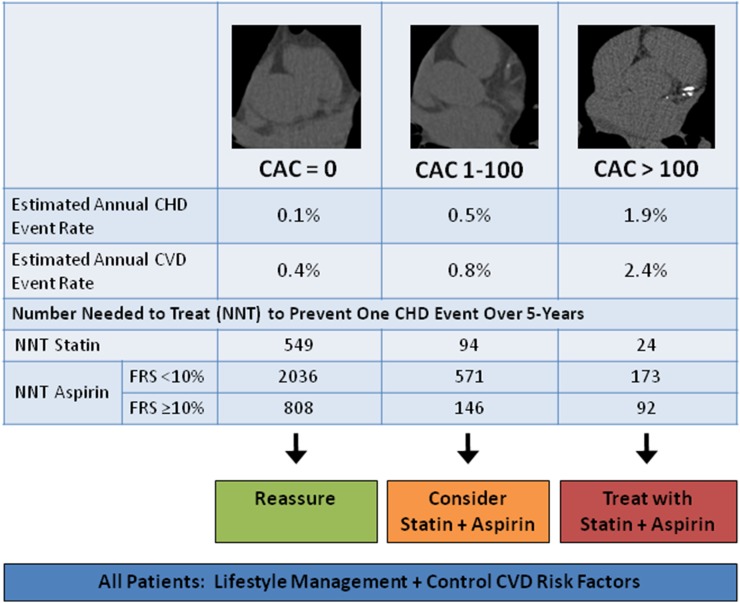
Coronary artery calcium (CAC) score prognosis and recommended treatment strategy. Note that the estimated number needed to harm with aspirin use is 442 patients to cause 1 major bleeding episode over a 5-year period. Thus, consider aspirin use in patients with CAC score of 1–100 when anticipated benefit exceeds risk [e.g., when Framingham risk score (FRS) ≥10%]. The amount of calcium is quantified using the Agatston score. CHD, coronary heart disease; CVD, cardiovascular disease.
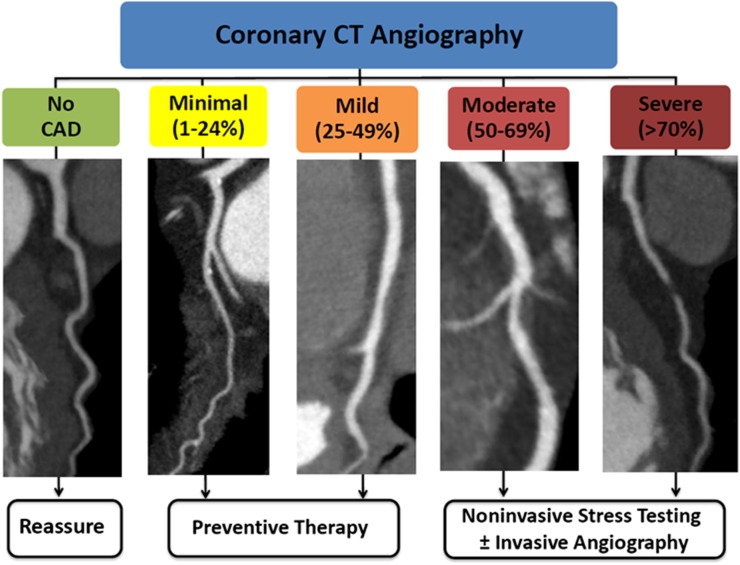
coronary artery disease (CAD) severity identified by coronary CT angiography and recommended management. Patients with a normal coronary CT angiography can be safely reassured. Follow-up for preventive therapy is recommended for non-obstructive (<50%) CAD. For obstructive CAD (≥50% stenosis), further testing is recommended to guide management. Adapted from Cheezum et al with permission from Informa Healthcare.
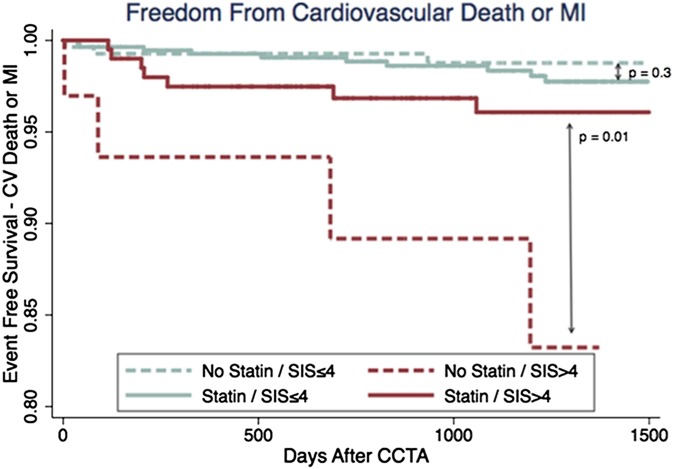
Event-free survival according to the presence or absence of statin therapy post-coronary CT angiography among patients with non-obstructive coronary artery disease, stratified by extent of disease according to segment involvement score (SIS). CCTA, coronary CT angiography; CV, cardiovascular; MI, myocardial infarction. Reproduced from Hulten et al with permission from Wolters Kluwer Health.
References
-
- Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 2001; 104: 2746–53. - PubMed
-
- National Cholesterol Education Program (NCEP) Expert Panel on Detection Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation 2002; 106: 3143–421. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation 2014; 129(Suppl. 2): S1–45. doi: 10.1161/01.cir.0000437738.63853.7a - DOI - PubMed
-
- Goff DC, Jr, Lloyd-Jones DM, Bennett G, Coady S, D'Agostino RB, Gibbons R, et al. ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation 2014; 129(Suppl. 2): S49–73. doi: 10.1161/01.cir.0000437741.48606.98 - DOI - PubMed
-
- Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M, et al. ; European Association for Cardiovascular Prevention & Rehabilitation (EACPR); ESC Committee for Practice Guidelines (CPG). European guidelines on cardiovascular disease prevention in clinical practice (version 2012). The fifth joint task force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts). Eur Heart J 2012; 33: 1635–701. doi: 10.1093/eurheartj/ehs092 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
