

Evaluation of quality improvement for cesarean sections caesarean section programmes through mixed methods
- PMID: 25496430
- PMCID: PMC4268855
- DOI: 10.1186/s13012-014-0182-0
Evaluation of quality improvement for cesarean sections caesarean section programmes through mixed methods
Erratum in
-
Erratum to: 'Evaluation of quality improvement for cesarean sections programmes through mixed methods'.Implement Sci. 2016 Mar 16;11:37. doi: 10.1186/s13012-016-0402-x. Implement Sci. 2016. PMID: 26984271 Free PMC article. No abstract available.
Abstract
Background: The rate of avoidable caesarean sections (CS) could be reduced through multifaceted strategies focusing on the involvement of health professionals and compliance with clinical practice guidelines (CPGs). Quality improvements for CS (QICS) programmes (QICS) based on this approach, have been implemented in Canada and Spain.
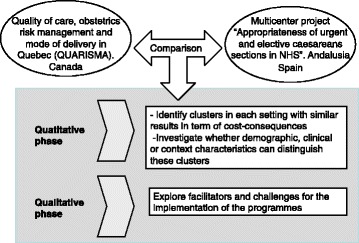
Objectives: Their objectives are as follows: 1) Toto identify clusters in each setting with similar results in terms of cost-consequences, 2) Toto investigate whether demographic, clinical or context characteristics can distinguish these clusters, and 3) Toto explore the implementation of QICS in the 2 regions, in order to identify factors that have been facilitators in changing practices and reducing the use of obstetric intervention, as well as the challenges faced by hospitals in implementing the recommendations.
Methods: Descriptive study with a quantitative and qualitative approach. 1) Cluster analysis at patient level with data from 16 hospitals in Quebec (Canada) (n = 105,348) and 15 hospitals in Andalusia (Spain) (n = 64,760). The outcome measures are CS and costs. For the cost, we will consider the intervention, delivery and complications in mother and baby, from the hospital perspective. Cluster analysis will be used to identify participants with similar patterns of CS and costs based, and t tests will be used to evaluate if the clusters differed in terms of characteristics: Hospital level (academic status of hospital, level of care, supply and demand factors), patient level (mother age, parity, gestational age, previous CS, previous pathology, presentation of the baby, baby birth weight). 2) Analysis of in-depth interviews with obstetricians and midwives in hospitals where the QICS were implemented, to explore the differences in delivery-related practices, and the importance of the different constructs for positive or negative adherence to CPGs. Dimensions: political/management level, hospital level, health professionals, mothers and their birth partner.
Discussion: This work sets out a new approach for programme evaluation, using different techniques to make it possible to take into account the specific context where the programmes were implemented.
Similar articles
-
A cluster-randomized trial to reduce caesarean delivery rates in Quebec: cost-effectiveness analysis.BMC Med. 2017 May 22;15(1):96. doi: 10.1186/s12916-017-0859-8. BMC Med. 2017. PMID: 28528578 Free PMC article. Clinical Trial.
-
Evaluation of a quality improvement intervention for labour and birth care in Brazilian private hospitals: a protocol.Reprod Health. 2018 Nov 26;15(1):194. doi: 10.1186/s12978-018-0636-y. Reprod Health. 2018. PMID: 30477517 Free PMC article.
-
SIMPLE: implementation of recommendations from international evidence-based guidelines on caesarean sections in the Netherlands. Protocol for a controlled before and after study.Implement Sci. 2013 Jan 3;8:3. doi: 10.1186/1748-5908-8-3. Implement Sci. 2013. PMID: 23281646 Free PMC article. Clinical Trial.
-
Evidence-based strategies for reducing cesarean section rates: a meta-analysis.Birth. 2007 Mar;34(1):53-64. doi: 10.1111/j.1523-536X.2006.00146.x. Birth. 2007. PMID: 17324180 Review.
-
Evidence-Based Strategies to Minimize Unnecessary Primary Cesarean Sections: A Comprehensive Review.Cureus. 2024 Nov 29;16(11):e74729. doi: 10.7759/cureus.74729. eCollection 2024 Nov. Cureus. 2024. PMID: 39735004 Free PMC article. Review.
Cited by
-
Improving the Caesarean Decision by Robson Classification: A Population-Based Study by 5,323,500 Livebirth Data.Ann Glob Health. 2020 Aug 17;86(1):101. doi: 10.5334/aogh.2615. Ann Glob Health. 2020. PMID: 32874932 Free PMC article.
-
Barriers and enablers in the implementation of a program to reduce cesarean deliveries.Reprod Health. 2017 Aug 29;14(1):106. doi: 10.1186/s12978-017-0369-3. Reprod Health. 2017. PMID: 28851394 Free PMC article.
-
Women's and communities' views of targeted educational interventions to reduce unnecessary caesarean section: a qualitative evidence synthesis.Reprod Health. 2018 Jul 24;15(1):130. doi: 10.1186/s12978-018-0570-z. Reprod Health. 2018. PMID: 30041661 Free PMC article.
-
What Are Optimal Cesarean Section Rates in the U.S. and How Do We Get There? A Review of Evidence-Based Recommendations and Interventions.J Womens Health (Larchmt). 2017 Dec;26(12):1285-1291. doi: 10.1089/jwh.2016.6188. Epub 2017 Aug 21. J Womens Health (Larchmt). 2017. PMID: 28825512 Free PMC article. Review.
-
Non-clinical interventions to reduce unnecessary caesarean section targeted at organisations, facilities and systems: Systematic review of qualitative studies.PLoS One. 2018 Sep 4;13(9):e0203274. doi: 10.1371/journal.pone.0203274. eCollection 2018. PLoS One. 2018. PMID: 30180198 Free PMC article.
References
-
- Allen VM, O'Connell CM, Liston RM, Baskett TF. Maternal morbidity associated with cesarean delivery without labor compared with spontaneous onset of labor at term. Obstet Gynecol. 2003;102(3):477–482. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
