

Comparing Open Radical Cystectomy and Robot-assisted Laparoscopic Radical Cystectomy: A Randomized Clinical Trial
- PMID: 25496767
- PMCID: PMC4424172
- DOI: 10.1016/j.eururo.2014.11.043
Comparing Open Radical Cystectomy and Robot-assisted Laparoscopic Radical Cystectomy: A Randomized Clinical Trial
Abstract
Background: Open radical cystectomy (ORC) and urinary diversion in patients with bladder cancer (BCa) are associated with significant perioperative complication risk.
Objective: To compare perioperative complications between robot-assisted radical cystectomy (RARC) and ORC techniques.
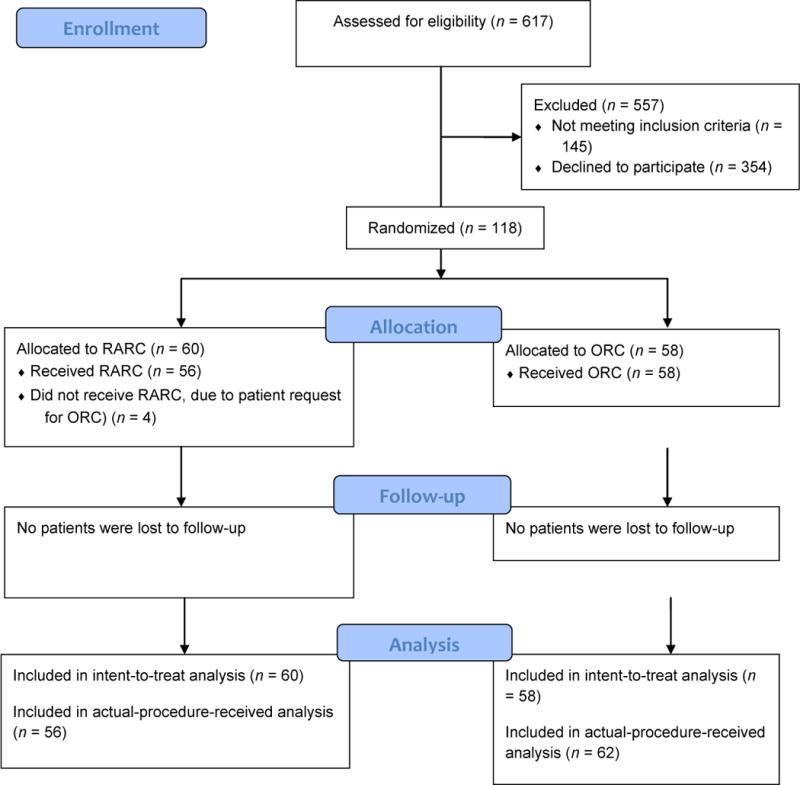
Design, setting, and participants: A prospective randomized controlled trial was conducted during 2010 and 2013 in BCa patients scheduled for definitive treatment by radical cystectomy (RC), pelvic lymph node dissection (PLND), and urinary diversion. Patients were randomized to ORC/PLND or RARC/PLND, both with open urinary diversion. Patients were followed for 90 d postoperatively.
Intervention: Standard ORC or RARC with PLND; all urinary diversions were performed via an open approach.
Outcome measurements and statistical analysis: Primary outcomes were overall 90-d grade 2-5 complications defined by a modified Clavien system. Secondary outcomes included comparison of high-grade complications, estimated blood loss, operative time, pathologic outcomes, 3- and 6-mo patient-reported quality-of-life (QOL) outcomes, and total operative room and inpatient costs. Differences in binary outcomes were assessed with the chi-square test, with differences in continuous outcomes assessed by analysis of covariance with randomization group as covariate and, for QOL end points, baseline score.
Results and limitations: The trial enrolled 124 patients, of whom 118 were randomized and underwent RC/PLND. Sixty were randomized to RARC and 58 to ORC. At 90 d, grade 2-5 complications were observed in 62% and 66% of RARC and ORC patients, respectively (95% confidence interval for difference, -21% to -13%; p=0.7). The similar rates of grade 2-5 complications at our mandated interim analysis met futility criteria; thus, early closure of the trial occurred. The RARC group had lower mean intraoperative blood loss (p=0.027) but significantly longer operative time than the ORC group (p<0.001). Pathologic variables including positive surgical margins and lymph node yields were similar. Mean hospital stay was 8 d in both arms (standard deviation, 3 and 5 d, respectively; p=0.5). Three- and 6-mo QOL outcomes were similar between arms. Cost analysis demonstrated an advantage to ORC compared with RARC. A limitation is the setting at a single high-volume, referral center; our findings may not be generalizable to all settings.
Conclusions: This trial failed to identify a large advantage for robot-assisted techniques over standard open surgery for patients undergoing RC/PLND and urinary diversion. Similar 90-d complication rates, hospital stay, pathologic outcomes, and 3- and 6-mo QOL outcomes were observed regardless of surgical technique.
Patient summary: Of 118 patients with bladder cancer who underwent radical cystectomy, pelvic lymph node dissection, and urinary diversion, half were randomized to open surgery and half to robot-assisted laparoscopic surgery. We compared the rate of complications within 90 d after surgery for the open group versus the robotic group and found no significant difference between the two groups.
Trial registration: ClinicalTrials.gov identifier NCT01076387, www.clinicaltrials.gov.
Keywords: Bladder cancer; Complications; Cystectomy; Lymph node dissection; Quality of life; Randomized controlled trial; Robot assisted; Robotic; Urinary diversion.
Copyright © 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
"The devil is in the details": randomized trial of robotic versus open radical cystectomy.Eur Urol. 2015 Jun;67(6):1053-1055. doi: 10.1016/j.eururo.2015.01.017. Epub 2015 Jan 29. Eur Urol. 2015. PMID: 25641689 No abstract available.
-
The surgeon makes the difference, not the instrument used.Eur Urol. 2015 Jun;67(6):1051-1052. doi: 10.1016/j.eururo.2015.01.018. Epub 2015 Jan 31. Eur Urol. 2015. PMID: 25650270 No abstract available.
-
Re: Comparing Open Radical Cystectomy and Robot-Assisted Laparoscopic Radical Cystectomy: A Randomized Clinical Trial.J Urol. 2015 Dec;194(6):1584-5. doi: 10.1016/j.juro.2015.09.006. Epub 2015 Sep 5. J Urol. 2015. PMID: 26582662 No abstract available.
-
Re: Comparing Open Radical Cystectomy and Robot-assisted Laparoscopic Radical Cystectomy: A Randomized Clinical Trial.Eur Urol. 2016 May;69(5):963-4. doi: 10.1016/j.eururo.2016.02.010. Eur Urol. 2016. PMID: 27301990 No abstract available.
References
-
- Chavan S, Bray F, Lortet-Tieulent J, Goodman M, Jemal A. International variations in bladder cancer incidence and mortality. Eur Urol. 2013;16:1074–9. - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Brennan P, Bogillot O, Cordier S, et al. Cigarette smoking and bladder cancer in men: a pooled analysis of 11 case-control studies. Int J Cancer. 2000;86:289–94. - PubMed
-
- Doll R, Peto R. The causes of cancer: quantitative estimates of avoidable risks of cancer in the United States today. J Natl Cancer Inst. 1981;66:1191–308. - PubMed
-
- Smith AB, Raynor M, Amling CL, et al. Multi-institutional analysis of robotic radical cystectomy for bladder cancer: perioperative outcomes and complications in 227 patients. J Laparoendosc Adv Surg Tech A. 2012;22:17–21. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
