

Refractory trigeminal neuralgia treatment outcomes following CyberKnife radiosurgery
- PMID: 25497053
- PMCID: PMC4273323
- DOI: 10.1186/s13014-014-0257-8
Refractory trigeminal neuralgia treatment outcomes following CyberKnife radiosurgery
Abstract
Introduction: A handful of studies have reported outcomes with CyberKnife radiosurgery (CKRS) for the treatment of trigeminal neuralgia. However, the follow-up has been short with no minimum follow-up required and have included patients with short duration of symptoms. Here we report our institutional experience on patients with a minimum follow-up of 1 year and a median follow-up of 28 months (mean 38.84 months).
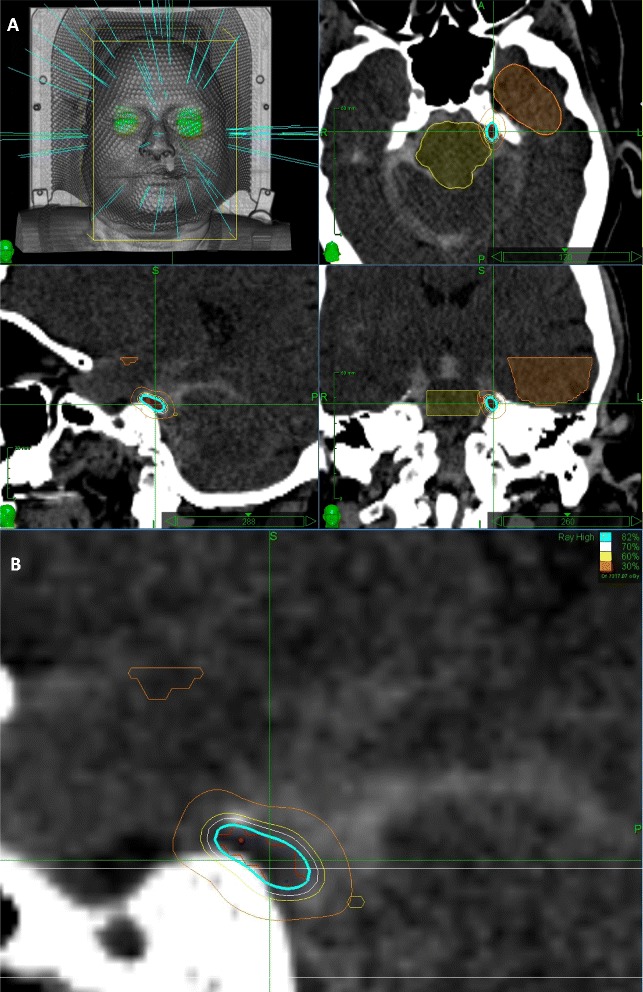
Methods: Twenty-five patients with medically and surgically intractable TN received CKRS with a mean marginal radiation dose of 64 Gy applied to an average isodose line of 86% of the affected trigeminal nerve. Follow-up data were obtained by clinical examination and telephone questionnaire. Outcome results were categorized based on the Barrow Neurological Institute (BNI) pain scale with BNI I-III considered to be good outcomes and BNI IV-V considered as treatment failure. BNI facial numbness score was used to assess treatment complications.
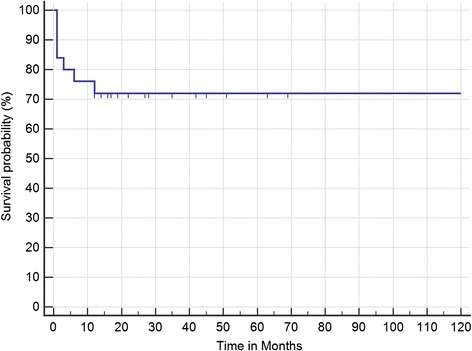
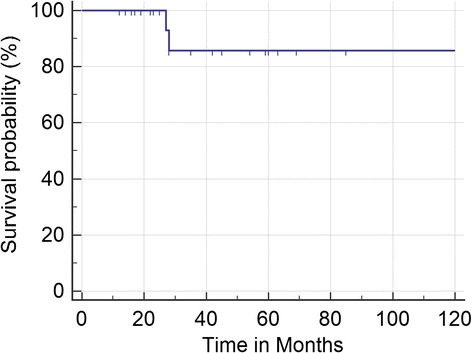
Results: A large proportion of patients (42.9%) reported pain relief within 1 month following CKRS treatment. The mean time to recurrence of severe pain was 27.8 months (range 1-129 months). At median follow-up of 28 months (mean 38.84 months), actuarial rate of freedom from severe pain (BNI ≥ III) was 72%. At last follow-up 2 (8%) patients had freedom from any pain and no medications (BNI I) and the majority (48%) had some pain that was adequately controlled with medications. Seven patients (28%) had no response to treatment and continued to suffer from severe pain (BNI IV or V). Patient's diabetic status and overall post-treatment BNI facial numbness scores were statistically significant predictors of treatment outcomes.
Conclusion: CKRS represents an acceptable salvage option for with medically and/or surgically refractory patients. Even patients with severely debilitating symptoms may experience significant and sustained pain relief after CKRS. Particularly, CKRS remains an attractive option in patients who are not good surgical candidates or possibly even failed surgical therapy. This data should help in setting realistic expectations for weighing the various available treatment options.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
