

Use of home telemonitoring to support multidisciplinary care of heart failure patients in Finland: randomized controlled trial
- PMID: 25498992
- PMCID: PMC4275484
- DOI: 10.2196/jmir.3651
Use of home telemonitoring to support multidisciplinary care of heart failure patients in Finland: randomized controlled trial
Abstract
Background: Heart failure (HF) patients suffer from frequent and repeated hospitalizations, causing a substantial economic burden on society. Hospitalizations can be reduced considerably by better compliance with self-care. Home telemonitoring has the potential to boost patients' compliance with self-care, although the results are still contradictory.
Objective: A randomized controlled trial was conducted in order to study whether the multidisciplinary care of heart failure patients promoted with telemonitoring leads to decreased HF-related hospitalization.
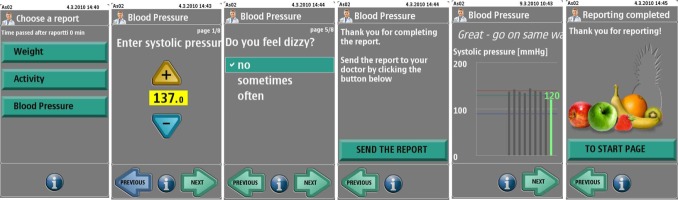
Methods: HF patients were eligible whose left ventricular ejection fraction was lower than 35%, NYHA functional class ≥2, and who needed regular follow-up. Patients in the telemonitoring group (n=47) measured their body weight, blood pressure, and pulse and answered symptom-related questions on a weekly basis, reporting their values to the heart failure nurse using a mobile phone app. The heart failure nurse followed the status of patients weekly and if necessary contacted the patient. The primary outcome was the number of HF-related hospital days. Control patients (n=47) received multidisciplinary treatment according to standard practices. Patients' clinical status, use of health care resources, adherence, and user experience from the patients' and the health care professionals' perspective were studied.
Results: Adherence, calculated as a proportion of weekly submitted self-measurements, was close to 90%. No difference was found in the number of HF-related hospital days (incidence rate ratio [IRR]=0.812, P=.351), which was the primary outcome. The intervention group used more health care resources: they paid an increased number of visits to the nurse (IRR=1.73, P<.001), spent more time at the nurse reception (mean difference of 48.7 minutes, P<.001), and there was a greater number of telephone contacts between the nurse and intervention patients (IRR=3.82, P<.001 for nurse-induced contacts and IRR=1.63, P=.049 for patient-induced contacts). There were no statistically significant differences in patients' clinical health status or in their self-care behavior. The technology received excellent feedback from the patient and professional side with a high adherence rate throughout the study.
Conclusions: Home telemonitoring did not reduce the number of patients' HF-related hospital days and did not improve the patients' clinical condition. Patients in the telemonitoring group contacted the Cardiology Outpatient Clinic more frequently, and on this way increased the use of health care resources.
Trial registration: Clinicaltrials.gov NCT01759368; http://clinicaltrials.gov/show/NCT01759368 (Archived by WebCite at http://www.webcitation.org/6UFxiCk8Z).
Keywords: EHFSBS; clinical outcomes; health care resources; heart failure; hospitalization; telemonitoring; user experience.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures


Similar articles
-
A Remote Medication Monitoring System for Chronic Heart Failure Patients to Reduce Readmissions: A Two-Arm Randomized Pilot Study.J Med Internet Res. 2016 Apr 17;18(5):e91. doi: 10.2196/jmir.5256. J Med Internet Res. 2016. PMID: 27154462 Free PMC article. Clinical Trial.
-
A remote monitoring and telephone nurse coaching intervention to reduce readmissions among patients with heart failure: study protocol for the Better Effectiveness After Transition - Heart Failure (BEAT-HF) randomized controlled trial.Trials. 2014 Apr 13;15:124. doi: 10.1186/1745-6215-15-124. Trials. 2014. PMID: 24725308 Free PMC article. Clinical Trial.
-
Outcomes of a Heart Failure Telemonitoring Program Implemented as the Standard of Care in an Outpatient Heart Function Clinic: Pretest-Posttest Pragmatic Study.J Med Internet Res. 2020 Feb 8;22(2):e16538. doi: 10.2196/16538. J Med Internet Res. 2020. PMID: 32027309 Free PMC article.
-
Accounting for Complexity in Home Telemonitoring: A Need for Context-Centred Evidence.Can J Cardiol. 2018 Jul;34(7):897-904. doi: 10.1016/j.cjca.2018.01.022. Epub 2018 Jan 31. Can J Cardiol. 2018. PMID: 29861204 Review.
-
Home Telemonitoring In Heart Failure: A Systematic Review And Meta-Analysis.Health Aff (Millwood). 2018 Dec;37(12):1983-1989. doi: 10.1377/hlthaff.2018.05087. Health Aff (Millwood). 2018. PMID: 30633680
Cited by
-
Exploring the Feasibility and Initial Impact of an mHealth-Based Disease Management Program for Chronic Ischemic Heart Disease: Formative Study.JMIR Form Res. 2024 Aug 22;8:e56380. doi: 10.2196/56380. JMIR Form Res. 2024. PMID: 39173150 Free PMC article.
-
The Effect of Noninvasive Telemonitoring for Chronic Heart Failure on Health Care Utilization: Systematic Review.J Med Internet Res. 2021 Sep 29;23(9):e26744. doi: 10.2196/26744. J Med Internet Res. 2021. PMID: 34586072 Free PMC article.
-
Non-Invasive Telemonitoring in Heart Failure: A Systematic Review.Medicina (Kaunas). 2025 Jul 15;61(7):1277. doi: 10.3390/medicina61071277. Medicina (Kaunas). 2025. PMID: 40731906 Free PMC article. Review.
-
Association of Adherence to Weight Telemonitoring With Health Care Use and Death: A Secondary Analysis of a Randomized Clinical Trial.JAMA Netw Open. 2020 Jul 1;3(7):e2010174. doi: 10.1001/jamanetworkopen.2020.10174. JAMA Netw Open. 2020. PMID: 32648924 Free PMC article. Clinical Trial.
-
Human-Centered Design of a Digital Health Tool to Promote Effective Self-care in Patients With Heart Failure: Mixed Methods Study.JMIR Form Res. 2022 May 10;6(5):e34257. doi: 10.2196/34257. JMIR Form Res. 2022. PMID: 35536632 Free PMC article.
References
-
- McMurray JJV, Stewart S. The burden of heart failure. Eur Heart J Suppl. 2002;4(suppleD):307–333.
-
- Lang CC, Mancini DM. Non-cardiac comorbidities in chronic heart failure. Heart. 2007 Jun;93(6):665–71. doi: 10.1136/hrt.2005.068296. http://europepmc.org/abstract/MED/16488925 - DOI - PMC - PubMed
-
- Chen J, Normand SL, Wang Y, Krumholz HM. National and regional trends in heart failure hospitalization and mortality rates for Medicare beneficiaries, 1998-2008. JAMA. 2011 Oct 19;306(15):1669–78. doi: 10.1001/jama.2011.1474. http://europepmc.org/abstract/MED/22009099 - DOI - PMC - PubMed
-
- Krumholz HM, Merrill AR, Schone EM, Schreiner GC, Chen J, Bradley EH, Wang Y, Wang Y, Lin Z, Straube BM, Rapp MT, Normand SL, Drye EE. Patterns of hospital performance in acute myocardial infarction and heart failure 30-day mortality and readmission. Circ Cardiovasc Qual Outcomes. 2009 Sep;2(5):407–13. doi: 10.1161/CIRCOUTCOMES.109.883256. http://circoutcomes.ahajournals.org/cgi/pmidlookup?view=long&pmid=20031870 - DOI - PubMed
-
- Desai AS, Stevenson LW. Rehospitalization for heart failure: predict or prevent? Circulation. 2012 Jul 24;126(4):501–6. doi: 10.1161/CIRCULATIONAHA.112.125435. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=22825412 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
