

Early high protein intake is associated with low mortality and energy overfeeding with high mortality in non-septic mechanically ventilated critically ill patients
- PMID: 25499096
- PMCID: PMC4279460
- DOI: 10.1186/s13054-014-0701-z
Early high protein intake is associated with low mortality and energy overfeeding with high mortality in non-septic mechanically ventilated critically ill patients
Abstract
Introduction: Early protein and energy feeding in critically ill patients is heavily debated and early protein feeding hardly studied.
Methods: A prospective database with mixed medical-surgical critically ill patients with prolonged mechanical ventilation (>72 hours) and measured energy expenditure was used in this study. Logistic regression analysis was used to analyse the relation between admission day-4 protein intake group (with cutoffs 0.8, 1.0, and 1.2 g/kg), energy overfeeding (ratio energy intake/measured energy expenditure > 1.1), and admission diagnosis of sepsis with hospital mortality after adjustment for APACHE II (Acute Physiology and Chronic Health Evaluation II) score.
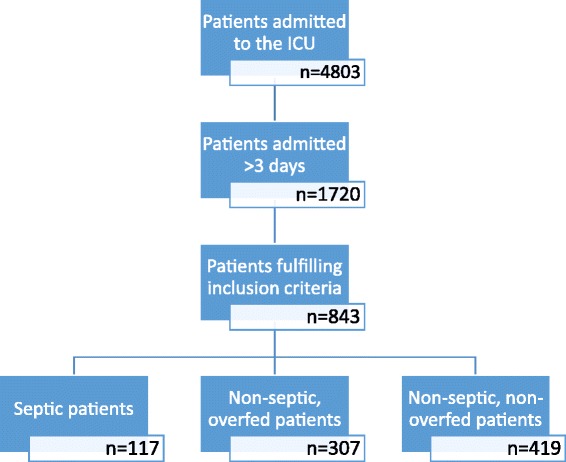
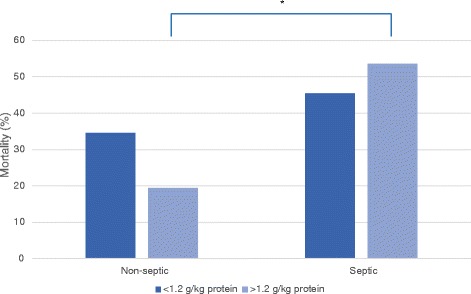
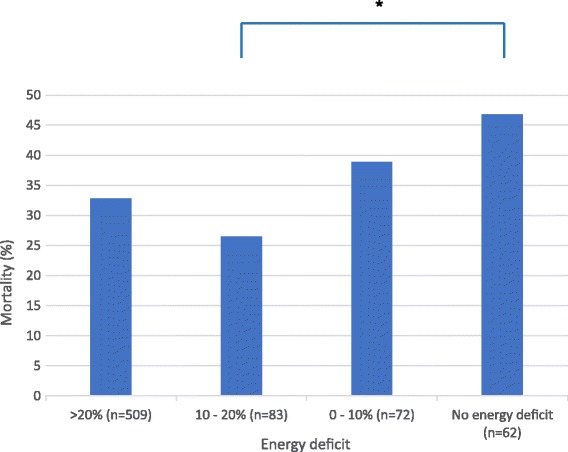
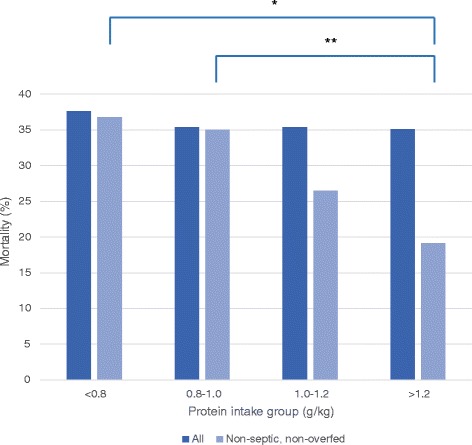
Results: A total of 843 patients were included. Of these, 117 had sepsis. Of the 736 non-septic patients 307 were overfed. Mean day-4 protein intake was 1.0 g/kg pre-admission weight per day and hospital mortality was 36%. In the total cohort, day-4 protein intake group (odds ratio (OR) 0.85; 95% confidence interval (CI) 0.73 to 0.99; P = 0.047), energy overfeeding (OR 1.62; 95%CI 1.07 to 2.44; P = 0.022), and sepsis (OR 1.77; 95%CI 1.18 to 2.65; P = 0.005) were independent risk factors for mortality besides APACHE II score. In patients with sepsis or energy overfeeding, day-4 protein intake was not associated with mortality. For non-septic, non-overfed patients (n = 419), mortality decreased with higher protein intake group: 37% for < 0.8 g/kg, 35% for 0.8 to 1.0 g/kg, 27% for 1.0 to 1.2 g/kg, and 19% for ≥ 1.2 g/kg (P = 0.033). For these, a protein intake level of ≥ 1.2 g/kg was significantly associated with lower mortality (OR 0.42, 95%CI 0.21 to 0.83, P = 0.013).
Conclusions: In non-septic critically ill patients, early high protein intake was associated with lower mortality and early energy overfeeding with higher mortality. In septic patients early high protein intake had no beneficial effect on mortality.
Figures
References
-
- Casaer MP, Mesotten D, Hermans G, Wouters PJ, Schetz M, Meyfroidt G, Van Cromphaut S, Ingels C, Meersseman P, Muller J, Vlasselaers D, Debaveye Y, Desmet L, Dubois J, Van Assche A, Vanderheyden S, Wilmer A, Van den Berghe G. Early versus late parenteral nutrition in critically ill adults. N Engl J Med. 2011;365:506–517. doi: 10.1056/NEJMoa1102662. - DOI - PubMed
-
- Doig GS, Simpson F, Sweetman EA, Finfer SR, Cooper DJ, Heighes PT, Davies AR, O’Leary M, Solano T, Peake S. Early parenteral nutrition in critically ill patients with short-term relative contraindications to early enteral nutrition: a randomized controlled trial. JAMA. 2013;309:2130–2138. doi: 10.1001/jama.2013.5124. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
