

Early versus delayed oral fluids and food for reducing complications after major abdominal gynaecologic surgery
- PMID: 25502897
- PMCID: PMC7044077
- DOI: 10.1002/14651858.CD004508.pub4
Early versus delayed oral fluids and food for reducing complications after major abdominal gynaecologic surgery
Update in
-
Early versus delayed oral feeding after major gynaecologic surgery.Cochrane Database Syst Rev. 2024 Aug 12;8(8):CD004508. doi: 10.1002/14651858.CD004508.pub5. Cochrane Database Syst Rev. 2024. PMID: 39132743 Free PMC article.
Abstract
Background: This is an updated version of the original Cochrane review published in 2007. Traditionally, after major abdominal gynaecologic surgery postoperative oral intake is withheld until the return of bowel function. There has been concern that early oral intake would result in vomiting and severe paralytic ileus with subsequent aspiration pneumonia, wound dehiscence, and anastomotic leakage. However, evidence-based clinical studies suggest that there may be benefits from early postoperative oral intake.
Objectives: To assess the effects of early versus delayed (traditional) initiation of oral intake of food and fluids after major abdominal gynaecologic surgery.
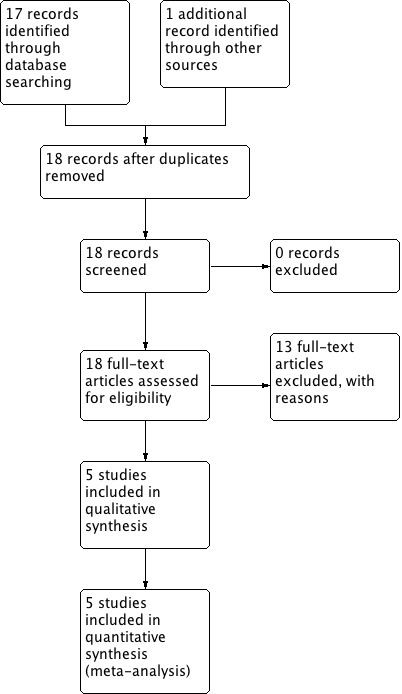
Search methods: We searched the Menstrual Disorders and Subfertility Group's Specialised Register, the Cochrane Central Register of Controlled Trials (CENTRAL), electronic databases (MEDLINE, EMBASE, CINAHL), and the citation lists of relevant publications. The most recent search was conducted 1 April 2014. We also searched a registry for ongoing trials (www.clinicaltrials.gov) on 13 May 2014.
Selection criteria: Randomised controlled trials (RCTs) were eligible that compared the effect of early versus delayed initiation of oral intake of food and fluids after major abdominal gynaecologic surgery. Early feeding was defined as oral intake of fluids or food within 24 hours post-surgery regardless of the return of bowel function. Delayed feeding was defined as oral intake after 24 hours post-surgery and only after signs of postoperative ileus resolution.
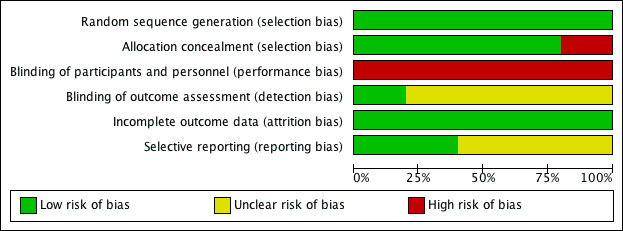
Data collection and analysis: Two review authors selected studies, assessed study quality and extracted the data. For dichotomous data, we calculated the risk ratio (RR) with a 95% confidence interval (CI). We examined continuous data using the mean difference (MD) and a 95% CI. We tested for heterogeneity between the results of different studies using a forest plot of the meta-analysis, the statistical tests of homogeneity of 2 x 2 tables and the I² value. We assessed the quality of the evidence using GRADE methods.
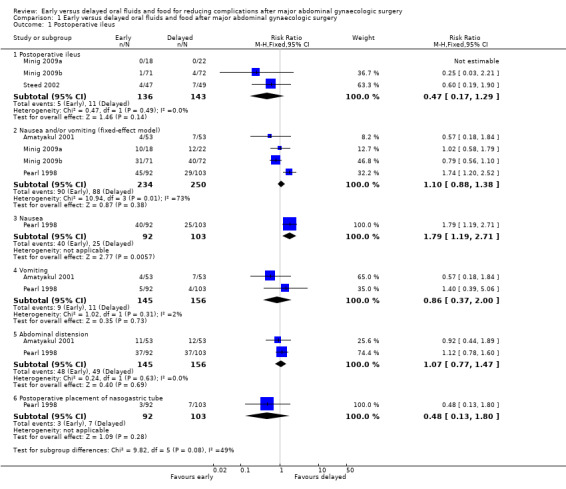
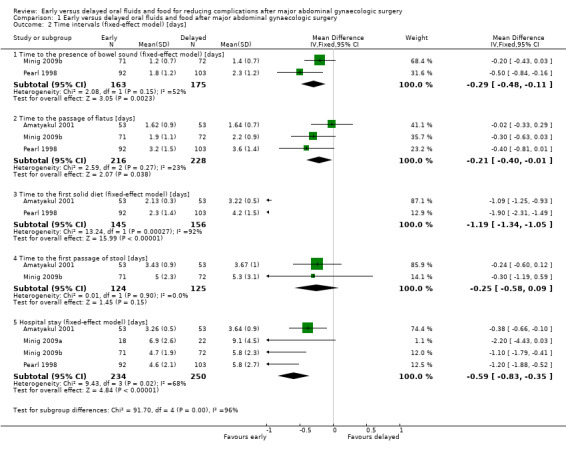
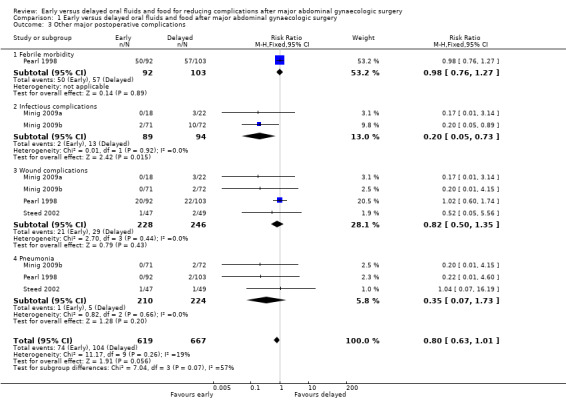
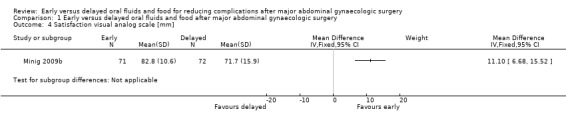
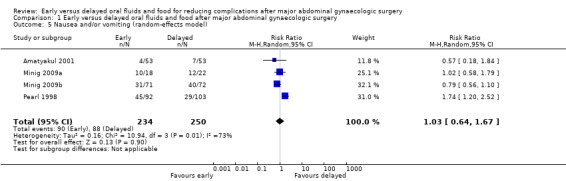
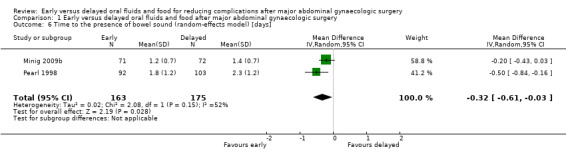
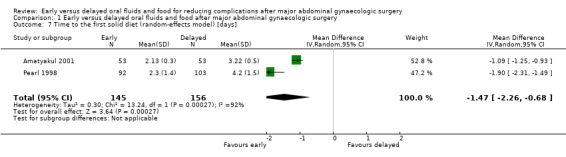
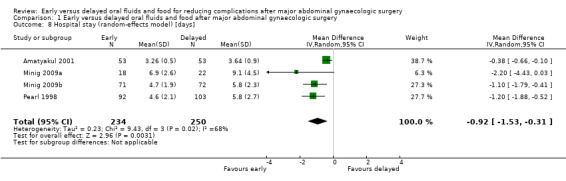
Main results: Rates of developing postoperative ileus were comparable between study groups (RR 0.47, 95% CI 0.17 to 1.29, P = 0.14, 3 RCTs, 279 women, I² = 0%, moderate-quality evidence). When we considered the rates of nausea or vomiting or both, there was no evidence of a difference between the study groups (RR 1.03, 95% CI 0.64 to 1.67, P = 0.90, 4 RCTs, 484 women, I² = 73%, moderate-quality evidence). There was no evidence of a difference between the study groups in abdominal distension (RR 1.07, 95% CI 0.77 to 1.47, 2 RCTs, 301 women, I² = 0%) or a need for postoperative nasogastric tube placement (RR 0.48, 95% CI 0.13 to 1.80, 1 RCT, 195 women).Early feeding was associated with shorter time to the presence of bowel sound (MD -0.32 days, 95% CI -0.61 to -0.03, P = 0.03, 2 RCTs, 338 women, I² = 52%, moderate-quality evidence) and faster onset of flatus (MD -0.21 days, 95% CI -0.40 to -0.01, P = 0.04, 3 RCTs, 444 women, I² = 23%, moderate-quality evidence). In addition, women in the early feeding group resumed a solid diet sooner (MD -1.47 days, 95% CI -2.26 to -0.68, P = 0.0003, 2 RCTs, 301 women, I² = 92%, moderate-quality evidence). There was no evidence of a difference in time to the first passage of stool between the two study groups (MD -0.25 days, 95% CI -0.58 to 0.09, P = 0.15, 2 RCTs, 249 women, I² = 0%, moderate-quality evidence). Hospital stay was shorter in the early feeding group (MD -0.92 days, 95% CI -1.53 to -0.31, P = 0.003, 4 RCTs, 484 women, I² = 68%, moderate-quality evidence). Infectious complications were less common in the early feeding group (RR 0.20, 95% CI 0.05 to 0.73, P = 0.02, 2 RCTs, 183 women, I² = 0%, high-quality evidence). In one study, the satisfaction score was significantly higher in the early feeding group (MD 11.10, 95% CI 6.68 to 15.52, P < 0.00001, 143 women, moderate-quality evidence).
Authors' conclusions: Early postoperative feeding after major abdominal gynaecologic surgery for either benign or malignant conditions appeared to be safe without increased gastrointestinal morbidities or other postoperative complications. The benefits of this approach include faster recovery of bowel function, lower rates of infectious complications, shorter hospital stay, and higher satisfaction.
Conflict of interest statement
Kittipat Charoenkwan: None Elizabeth Matovinovic: None
Figures
Update of
-
Early versus delayed (traditional) oral fluids and food for reducing complications after major abdominal gynaecologic surgery.Cochrane Database Syst Rev. 2007 Oct 17;(4):CD004508. doi: 10.1002/14651858.CD004508.pub3. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2014 Dec 12;(12):CD004508. doi: 10.1002/14651858.CD004508.pub4. PMID: 17943817 Updated.
References
References to studies included in this review
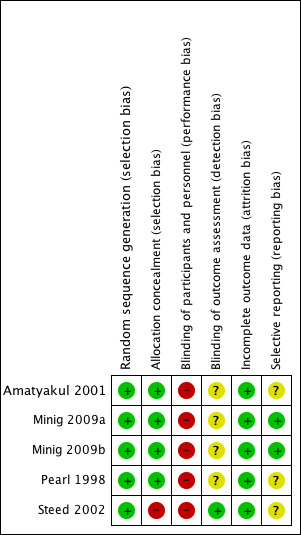
Amatyakul 2001 {unpublished data only}
-
- Amatyakul P, Suprasert P. Length of hospital stay after major gynecologic operation: a comparison between traditional and early oral feeding. Dissertation thesis for the diploma in Obstetrics and Gynecology, The Royal Thai College of Obstetricians and Gynecologists 2001.
Minig 2009a {published data only}
-
- Minig L, Biffi R, Zanagnolo V, Attanasio A, Beltrami C, Bocciolone L, et al. Early oral versus "traditional" postoperative feeding in gynecologic oncology patients undergoing intestinal resection: a randomized controlled trial. Annals of Surgical Oncology 2009;16(6):1660‐8. - PubMed
Minig 2009b {published data only}
-
- Minig L, Biffi R, Zanagnolo V, Attanasio A, Beltrami C, Bocciolone L, et al. Reduction of postoperative complication rate with the use of early oral feeding in gynecologic oncologic patients undergoing a major surgery: a randomized controlled trial. Annals of Surgical Oncology 2009;16(11):3101‐10. - PubMed
Pearl 1998 {published data only}
-
- Pearl ML, Valea FA, Fischer M, Mahler L, Chalas E. A randomized controlled trial of early postoperative feeding in gynecologic oncology patients undergoing intra‐abdominal surgery. Obstetrics and Gynecology 1998;92(1):94‐7. - PubMed
Steed 2002 {published data only}
-
- Steed HL, Capstick V, Flood C, Schepansky A, Schulz J, Mayes DC. A randomized controlled trial of early versus "traditional" postoperative oral intake after major abdominal gynecologic surgery. American Journal of Obstetrics and Gynecology 2002;186(5):861‐5. - PubMed
References to studies excluded from this review
Cutillo 1999 {published data only}
-
- Cutillo G, Maneschi F, Franchi M, Giannice R, Scambia G, Benedetti‐Panici P. Early feeding compared with nasogastric decompression after major oncologic gynecologic surgery: a randomized study. Obstetrics and Gynecology 1999;93(1):41‐5. - PubMed
Delaney 2005 {published data only}
-
- Delaney C, Weese J, Hyman N, Bauer J, Techner L, Gabriel K, Du W, Schmidt W, Wallin B. Phase III trial of alvimopan, a novel, peripherally acting, Mu opioid antagonist, for postoperative ileus after major abdominal surgery. Diseases of the Colon and Rectum 2005;48(6):1114‐29. - PubMed
Fanning 1999 {published data only}
-
- Fanning J, Yu‐Brekke S. Prospective trial of aggressive postoperative bowel stimulation following radical hysterectomy. Gynecologic Oncology 1999;73(3):412‐4. - PubMed
Fanning 2011 {published data only}
-
- Fanning J, Hojat R. Safety and efficacy of immediate postoperative feeding and bowel stimulation to prevent ileus after major gynecologic surgical procedures. Journal of the American Osteopathic Association 2011;111(8):469‐72. - PubMed
Feng 2008 {published data only}
-
- Feng S, Chen L, Wang G, Chen A, Qiu Y. Early oral intake after intra‐abdominal gynecological oncology surgery. Cancer Nursing 2008;31(3):209‐13. - PubMed
Finan 1995 {published data only}
-
- Finan M, Barton D, Fiorica J, Hoffman M, Roberts W, Gleeson N, et al. Ileus following gynecologic surgery: management with water‐soluble hyperosmolar radiocontrast material. Southern Medical Journal 1995;88(5):539‐42. - PubMed
Griffenberg 1997 {published data only}
-
- Griffenberg L, Morris M, Atkinson N, Levenback C. The effect of dietary fiber on bowel function following radical hysterectomy: a randomized trial. Gynecologic Oncology 1997;66(3):417‐24. - PubMed
Kraus 2000 {published data only}
-
- Kraus K, Fanning J. Prospective trial of early feeding and bowel stimulation after radical hysterectomy. American Journal of Obstetrics and Gynecology 2000;182(5):996‐8. - PubMed
MacMillan 2000 {published data only}
-
- MacMillan SL, Kammerer‐Doak D, Rogers RG, Parker KM. Early feeding and the incidence of gastrointestinal symptoms after major gynecologic surgery. Obstetrics and Gynecology 2000;96(4):604‐8. - PubMed
Pearl 2002 {published data only}
-
- Pearl ML, Frandina M, Mahler L, Valea FA, DiSilvestro PA, Chalas E. A randomized controlled trial of a regular diet as the first meal in gynecologic oncology patients undergoing intraabdominal surgery. Obstetrics and Gynecology 2002;100(2):230‐4. - PubMed
Schilder 1997 {published data only}
-
- Schilder JM, Hurteau JA, Look KY, Moore DH, Raff G, Stehman FB, et al. A prospective controlled trial of early postoperative oral intake following major abdominal gynecologic surgery. Gynecologic Oncology 1997;67(3):235‐40. - PubMed
Taguchi 2001 {published data only}
-
- Taguchi A, Sharma N, Saleem R, Sessler D, Carpenter R, Seyedsadr M, et al. Selective postoperative inhibition of gastrointestinal opioid receptors. New England Journal of Medicine 2001;345(13):935‐40. - PubMed
Terzioglu 2013 {published data only}
-
- Terzioglu F, Şimsek S, Karaca K, Sariince N, Altunsoy P, Salman MC. Multimodal interventions (chewing gum, early oral hydration and early mobilisation) on the intestinal motility following abdominal gynaecologic surgery. Journal of Clinical Nursing 2013;22(13‐14):1917‐25. - PubMed
Additional references
Bufo 1994
-
- Bufo AJ, Feldman S, Daniels GA, Lieberman RC. Early postoperative feeding. Dis Colon Rectum 1994;37:1260‐5. - PubMed
Deitch 1991
-
- Deitch EA, Andrassy RJ, Booth FVM, Moore FA. Current concepts in postoperative feeding. Contemporary Surgery 1991;39:37‐55.
Fanning 2001
-
- Fanning J, Andrews S. Early postoperative feeding after major gynecologic surgery: evidence‐based scientific medicine. American Journal of Obstetrics and Gynecology 2001;185(1):1‐4. - PubMed
Higgins 2003
Higgins 2011
-
- Higgins JPT, Altman DG, Sterne JAC. Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Kelly 1997
-
- Kelly DG, Stanhope CR. Postoperative enteral feeding: myth or fact?. Gynecol Oncol 1997;67:233‐4. - PubMed
Lewis 2001
Mangesi 2002
Nachlas 1972
Reissman 1995
Singh 1998
-
- Singh G, Ram RP, Khanna SK. Early postoperative enteral feeding in patients with nontraumatic intestinal perforation and peritonitis. Journal of the American College of Surgeons 1998;187(2):142‐6. - PubMed
Wells 1964
-
- Wells C, Tinckler LF, Rawlinson K, Jones H, Saunders J. Post‐operative gastrointestinal motility. Lancet 1964;I(7323):4‐10. - PubMed
Wilson 1975
Windsor 1988
-
- Windsor JA, Knight GS, Hill GL. Wound healing response in surgical patients: recent food intake is more important than nutritional status. British Journal of Surgery 1988;75(2):135‐7. - PubMed
Woods 1978
-
- Woods JH, Erickson LW, Condon RE, Schulte WJ, Sillin LE. Post‐operative ileus. A colonic problem?. Surgery 1978;84(4):527‐33. - PubMed
References to other published versions of this review
Charoenkwan 2003
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous