

Oropharyngeal aspiration of Burkholderia mallei and Burkholderia pseudomallei in BALB/c mice
- PMID: 25503969
- PMCID: PMC4263729
- DOI: 10.1371/journal.pone.0115066
Oropharyngeal aspiration of Burkholderia mallei and Burkholderia pseudomallei in BALB/c mice
Abstract
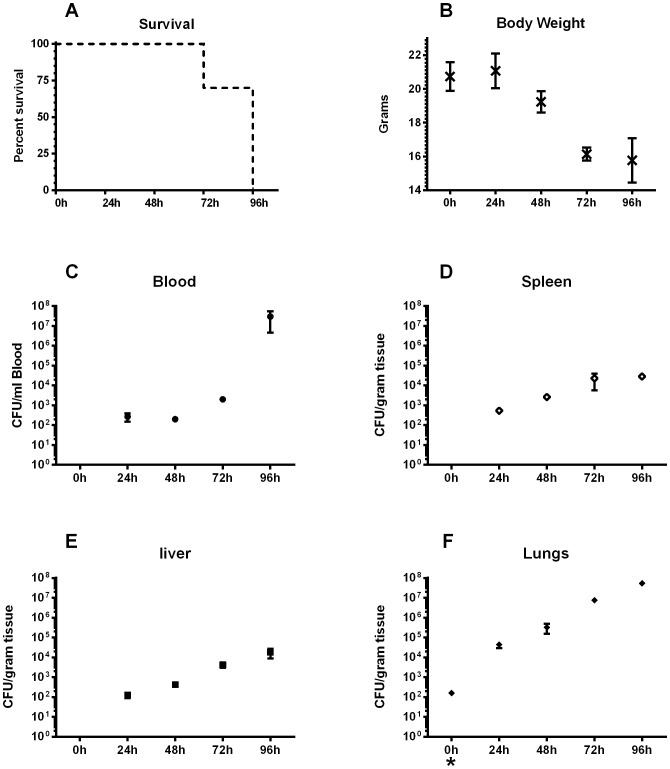
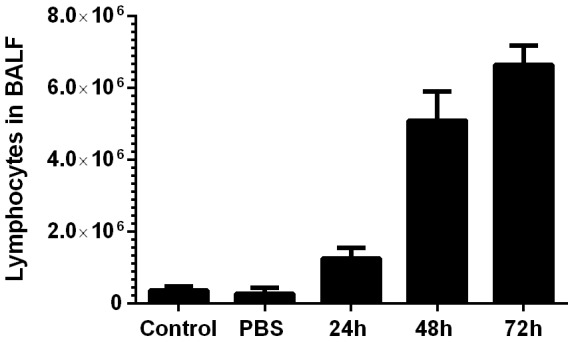
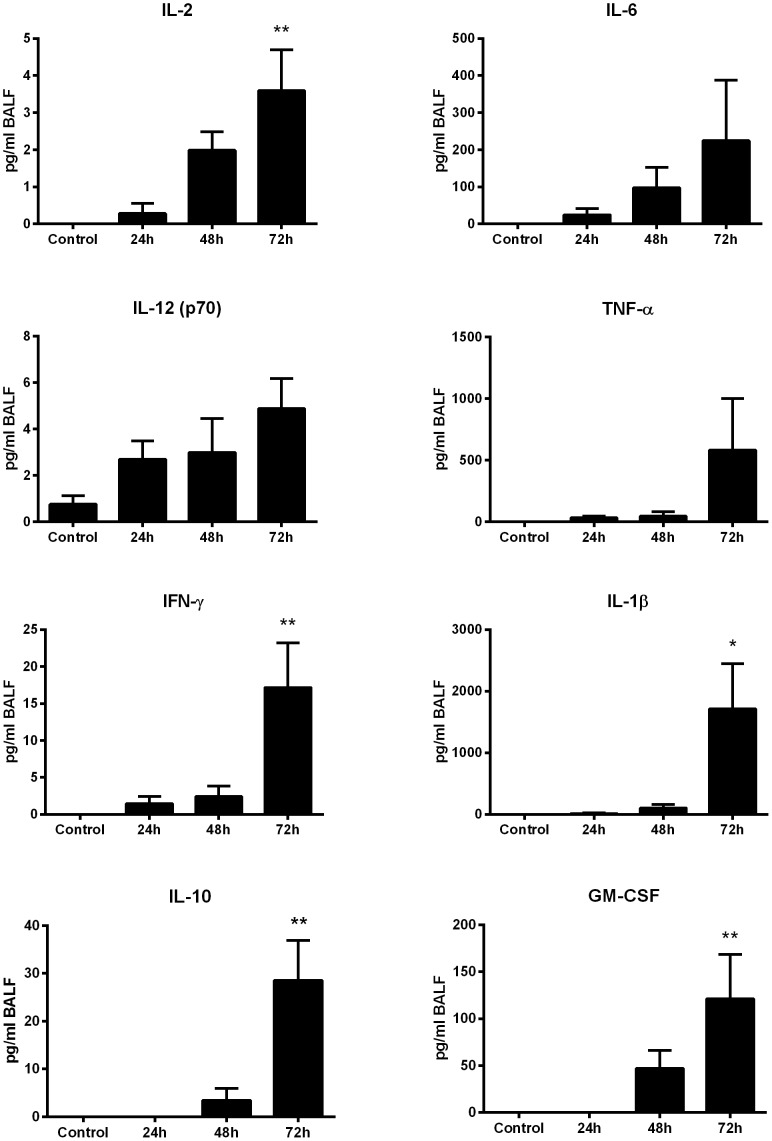
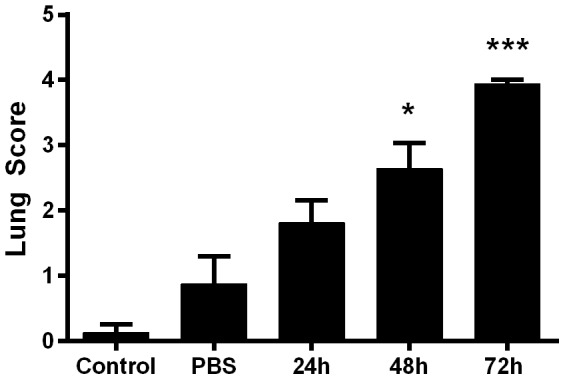
Burkholderia mallei and Burkholderia pseudomallei are potentially lethal pathogens categorized as biothreat agents due, in part, to their ability to be disseminated via aerosol. There are no protective vaccines against these pathogens and treatment options are limited and cumbersome. Since disease severity is greatest when these agents are inhaled, efforts to develop pre- or post-exposure prophylaxis focus largely on inhalation models of infection. Here, we demonstrate a non-invasive and technically simple method for affecting the inhalational challenge of BALB/c mice with B. pseudomallei and B. mallei. In this model, two investigators utilized common laboratory tools such as forceps and a micropipette to conduct and characterize an effective and reproducible inhalational challenge of BALB/c mice with B. mallei and B. pseudomallei. Challenge by oropharyngeal aspiration resulted in acute disease. Additionally, 50% endpoints for B. pseudomallei K96243 and B. mallei ATCC 23344 were nearly identical to published aerosol challenge methods. Furthermore, the pathogens disseminated to all major organs typically targeted by these agents where they proliferated. The pro-inflammatory cytokine production in the proximal and peripheral fluids demonstrated a rapid and robust immune response comparable to previously described murine and human studies. These observations demonstrate that OA is a viable alternative to aerosol exposure.
Conflict of interest statement
Figures
Similar articles
-
Use of a safe, reproducible, and rapid aerosol delivery method to study infection by Burkholderia pseudomallei and Burkholderia mallei in mice.PLoS One. 2013 Oct 2;8(10):e76804. doi: 10.1371/journal.pone.0076804. eCollection 2013. PLoS One. 2013. PMID: 24098563 Free PMC article.
-
Antibodies against In Vivo-Expressed Antigens Are Sufficient To Protect against Lethal Aerosol Infection with Burkholderia mallei and Burkholderia pseudomallei.Infect Immun. 2017 Jul 19;85(8):e00102-17. doi: 10.1128/IAI.00102-17. Print 2017 Aug. Infect Immun. 2017. PMID: 28507073 Free PMC article.
-
Relationship between antigenicity and pathogenicity for Burkholderia pseudomallei and Burkholderia mallei revealed by a large panel of mouse MAbs.Hybridoma (Larchmt). 2008 Aug;27(4):231-40. doi: 10.1089/hyb.2008.0012. Hybridoma (Larchmt). 2008. PMID: 18707541
-
Development of Burkholderia mallei and pseudomallei vaccines.Front Cell Infect Microbiol. 2013 Mar 11;3:10. doi: 10.3389/fcimb.2013.00010. eCollection 2013. Front Cell Infect Microbiol. 2013. PMID: 23508691 Free PMC article. Review.
-
Molecular insights into Burkholderia pseudomallei and Burkholderia mallei pathogenesis.Annu Rev Microbiol. 2010;64:495-517. doi: 10.1146/annurev.micro.112408.134030. Annu Rev Microbiol. 2010. PMID: 20528691 Review.
Cited by
-
Evaluation of a temperature-restricted, mucosal tuberculosis vaccine in guinea pigs.Tuberculosis (Edinb). 2018 Dec;113:179-188. doi: 10.1016/j.tube.2018.10.006. Epub 2018 Oct 19. Tuberculosis (Edinb). 2018. PMID: 30514501 Free PMC article.
-
Oropharyngeal aspiration of bleomycin: An alternative experimental model of pulmonary fibrosis developed in Swiss mice.Indian J Pharmacol. 2016 Nov-Dec;48(6):643-648. doi: 10.4103/0253-7613.194859. Indian J Pharmacol. 2016. PMID: 28066100 Free PMC article.
-
Burkholderia pseudomallei ΔtonB Δhcp1 Live Attenuated Vaccine Strain Elicits Full Protective Immunity against Aerosolized Melioidosis Infection.mSphere. 2019 Jan 2;4(1):e00570-18. doi: 10.1128/mSphere.00570-18. mSphere. 2019. PMID: 30602524 Free PMC article.
-
Assessment of the Virulence of the Burkholderia mallei Strain BAC 86/19 in BALB/c Mice.Microorganisms. 2023 Oct 20;11(10):2597. doi: 10.3390/microorganisms11102597. Microorganisms. 2023. PMID: 37894255 Free PMC article.
-
Distinct roles for type I and type III interferons in virulent human metapneumovirus pathogenesis.PLoS Pathog. 2024 Feb 5;20(2):e1011840. doi: 10.1371/journal.ppat.1011840. eCollection 2024 Feb. PLoS Pathog. 2024. PMID: 38315735 Free PMC article.
References
-
- Stanton AT, Fletcher W (1921) Melioidosis, a new disease of the tropics. Trans Fourth Congr Far East Assoc Trop Med Hyg. Batavia 2:196–198.
-
- Currie BJ, Dance DA, Cheng AC (2008) The global distribution of Burkholderia pseudomallei and melioidosis: an update. Trans R Soc Trop Med Hyg 102 Suppl 1S1–4. - PubMed
-
- Chaowagul W, White NJ, Dance DA, Wattanagoon Y, Naigowit P, et al. (1989) Melioidosis: a major cause of community-acquired septicemia in northeastern Thailand. J Infect Dis 159:890–899. - PubMed
-
- Boonsawat W, Boonma P, Tangdajahiran T, Paupermpoonsiri S, Wongpratoom W, et al. (1990) Community-acquired pneumonia in adults at Srinagarind Hospital. J Med Assoc Thai 73:345–352. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
