

Beyond broken spines-what the radiologist needs to know about late complications of spinal cord injury
- PMID: 25503997
- PMCID: PMC4330228
- DOI: 10.1007/s13244-014-0375-8
Beyond broken spines-what the radiologist needs to know about late complications of spinal cord injury
Abstract
Objective: To describe expected imaging findings to assist the emergency room radiologist with recognising complications and pathology unique to the spinal cord injury (SCI) patient population to ensure rapid and accurate diagnosis.
Methods: Pictorial review.
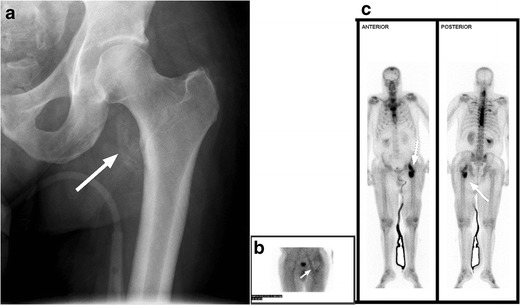
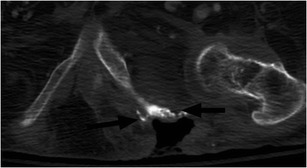
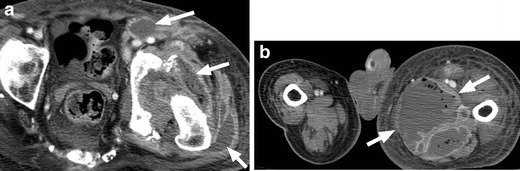
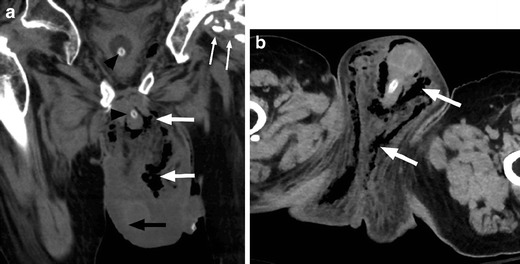
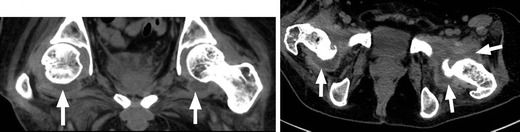
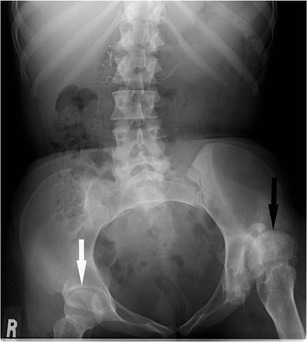
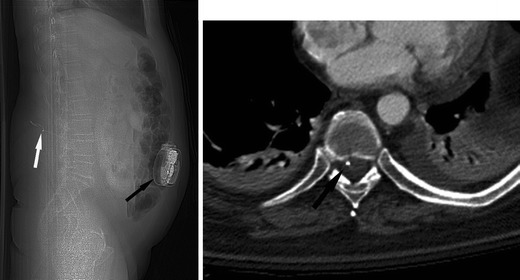
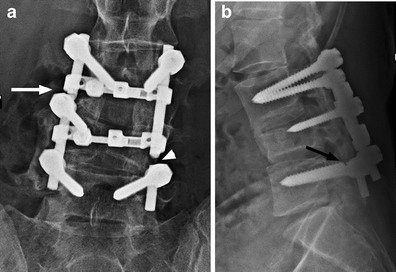
Results: We review several imaging findings common to persons with chronic SCI, emphasising imaging in the emergency setting and on CT.
Conclusion: SCI patients present a unique diagnostic challenge, as they may present with symptoms that are difficult to localise because of abnormal sensation and autonomic instability. Imaging plays an important role in the emergent setting, rapidly differentiating the most commonly encountered complications from less common, unanticipated complications. Radiologists need to be attuned to both the expected findings and potential complications, which may be unique to SCI patients, to ensure accurate diagnosis and treatment in the emergency setting.
Main messages: • Medical complications after spinal cord injury are common and associated with significant morbidity. • Radiologists should be aware of complications unique to the SCI population to aid diagnosis. • Due to abnormal sensation, SCI patients often present with symptoms that are difficult to localise. • In the ED, imaging helps to rapidly differentiate common complications from less anticipated ones.
Figures






References
-
- Spinal cord injury facts and figures at a glance. National Spinal Cord Injury Statistical Center, Birminham AL. Feb 2011. https://www.nscisc.uab.edu.
LinkOut - more resources
Full Text Sources
Other Literature Sources
