

Serum sodium and survival benefit of liver transplantation
- PMID: 25504743
- PMCID: PMC4354811
- DOI: 10.1002/lt.24063
Serum sodium and survival benefit of liver transplantation
Abstract
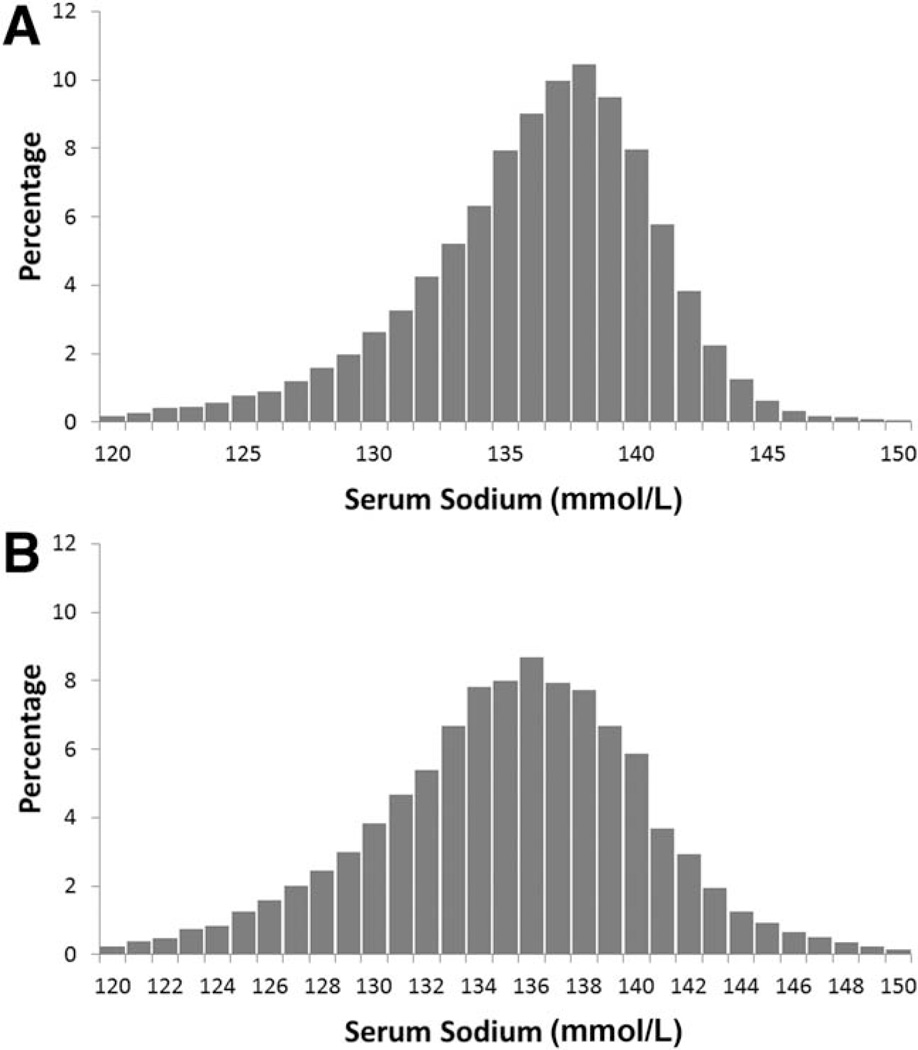
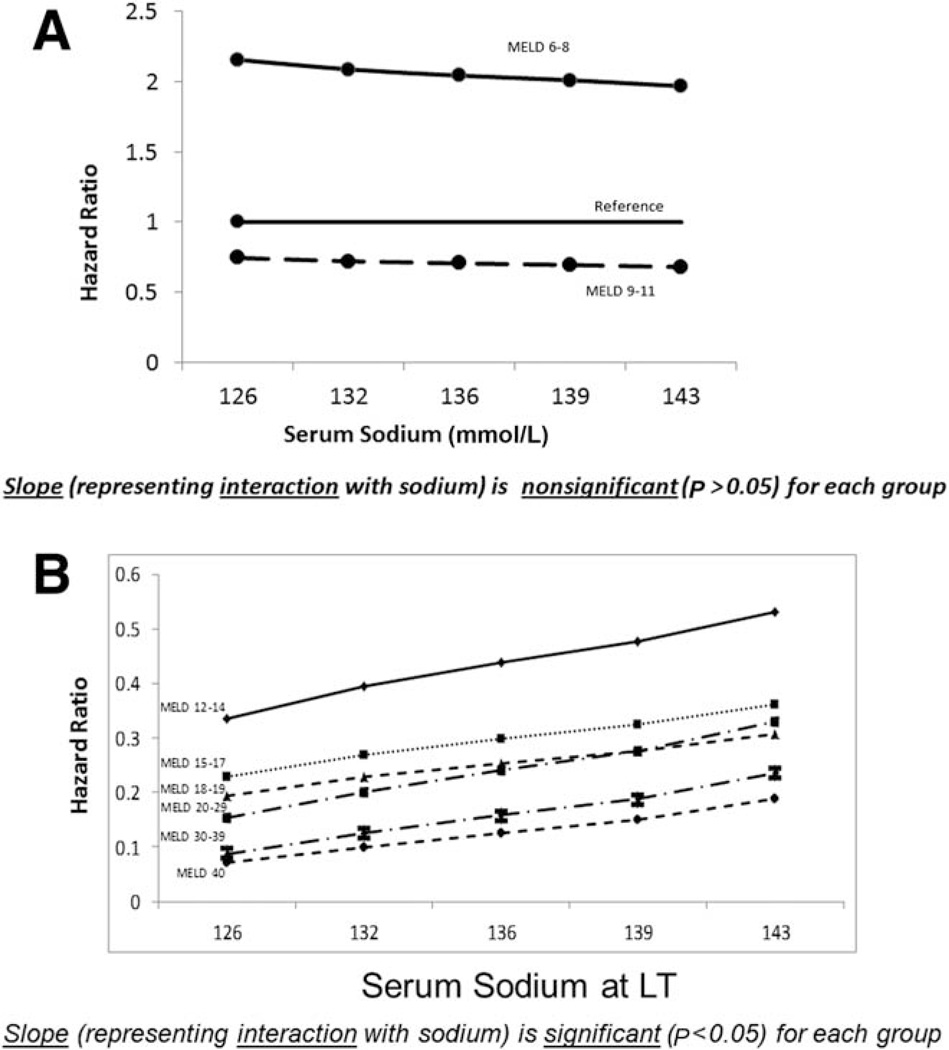
Hyponatremia is associated with elevated wait-list mortality among end-stage liver disease candidates for liver transplantation (LT). However, the effect of low serum sodium on the survival benefit of LT has not been examined. We sought to determine whether pretransplant hyponatremia is associated with an altered LT survival benefit. Data were obtained from the Scientific Registry of Transplant Recipients. The study population consisted of adults (age ≥ 18 years) placed on the waiting list for LT between January 1, 2005 and December 31, 2012 (n = 69,213). The effect of hyponatremia on the survival benefit was assessed via sequential stratification, an extension of Cox regression. Each transplant recipient was matched to appropriate candidates then active on the waiting list with the same Model for End-Stage Liver Disease (MELD) score and in the same donation service area. The focus of the analysis was the interaction between the serum sodium and the MELD score with respect to the survival benefit of LT; this was defined as the covariate-adjusted hazard ratio contrasting post-LT mortality and pre-LT mortality. The LT survival benefit increased significantly with decreasing serum sodium values when the MELD scores were >11. The survival benefit of LT was not affected by serum sodium for patients with MELD scores ≤ 11. In conclusion, the LT survival benefit (or lack thereof) is independent of serum sodium for patients with MELD scores ≤ 11. The increase in the survival benefit with decreasing serum sodium among patients with MELD scores > 11 is consistent with recently approved changes to the allocation system incorporating serum sodium.
© 2015 American Association for the Study of Liver Diseases.
Conflict of interest statement
Potential conflict of interest: Nothing to report.
Figures
Comment in
-
Use of serum sodium for liver transplant graft allocation: a decade in the making, now is it ready for primetime?Liver Transpl. 2015 Mar;21(3):279-81. doi: 10.1002/lt.24085. Liver Transpl. 2015. PMID: 25641769 No abstract available.
References
-
- Institute of Medicine. Organ Procurement and Transplantation: Assessing Current Policies and the Potential Impact of the DHHS Final Rule. Washington, DC: National Academies Press; 1999. Analysis of waiting times; pp. 61–90. - PubMed
-
- Wiesner RH, McDiarmid SV, Kamath PS, Edwards EB, Malinchoc M, Kremers WK, et al. MELD and PELD: application of survival models to liver allocation. Liver Transpl. 2001;7:567–580. - PubMed
-
- Wiesner R, Edwards E, Freeman R, Harper A, Kim R, Kamath P, et al. for United Network for Organ Sharing Liver Disease Severity Score Committee. Model for End-Stage Liver Disease (MELD) and allocation of donor livers. Gastroenterology. 2003;124:91–96. - PubMed
-
- Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33:464–470. - PubMed
-
- Organ Procurement and Transplantation Network. Policy 9: allocation of livers and liver-intestines. [Accessed November 2014]; http://optn.transplant.hrsa.gov/ContentDocuments/OPTN_Policies.pdf.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical