

A prospective study of severe irritability in youths: 2- and 4-year follow-up
- PMID: 25504765
- PMCID: PMC10530700
- DOI: 10.1002/da.22336
A prospective study of severe irritability in youths: 2- and 4-year follow-up
Abstract
Background: Severe, chronic irritability is receiving increased research attention, and is the cardinal symptom of a new diagnostic category, disruptive mood dysregulation disorder (DMDD). Although data from epidemiological community samples suggest that childhood chronic irritability predicts unipolar depression and anxiety in adulthood, whether these symptoms are stable and cause ongoing clinical impairment is unknown. The present study presents 4-year prospective and longitudinal diagnostic and impairment data on a clinical sample of children selected for symptoms of severe irritability (operationalized as severe mood dysregulation [SMD]).
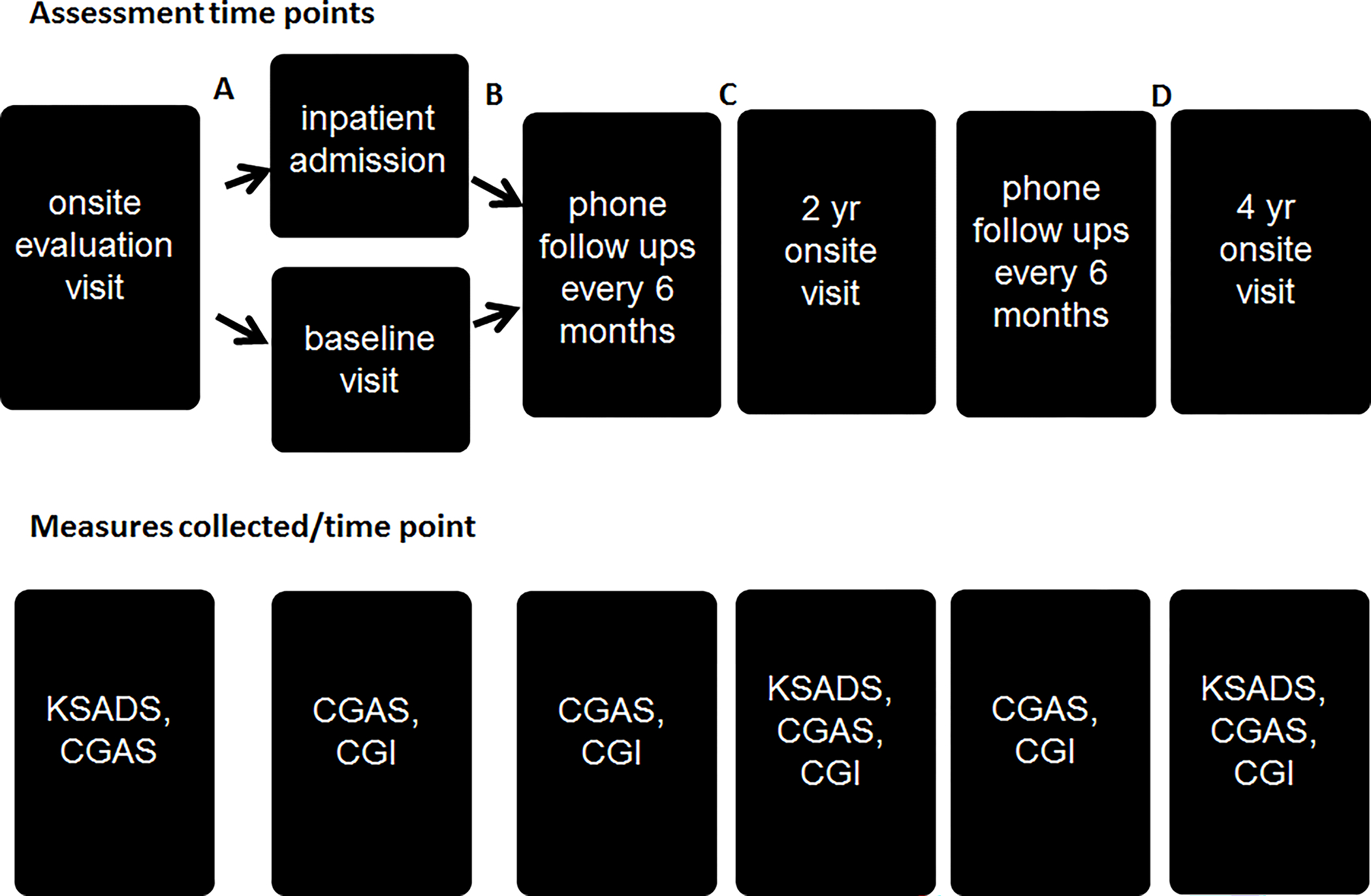
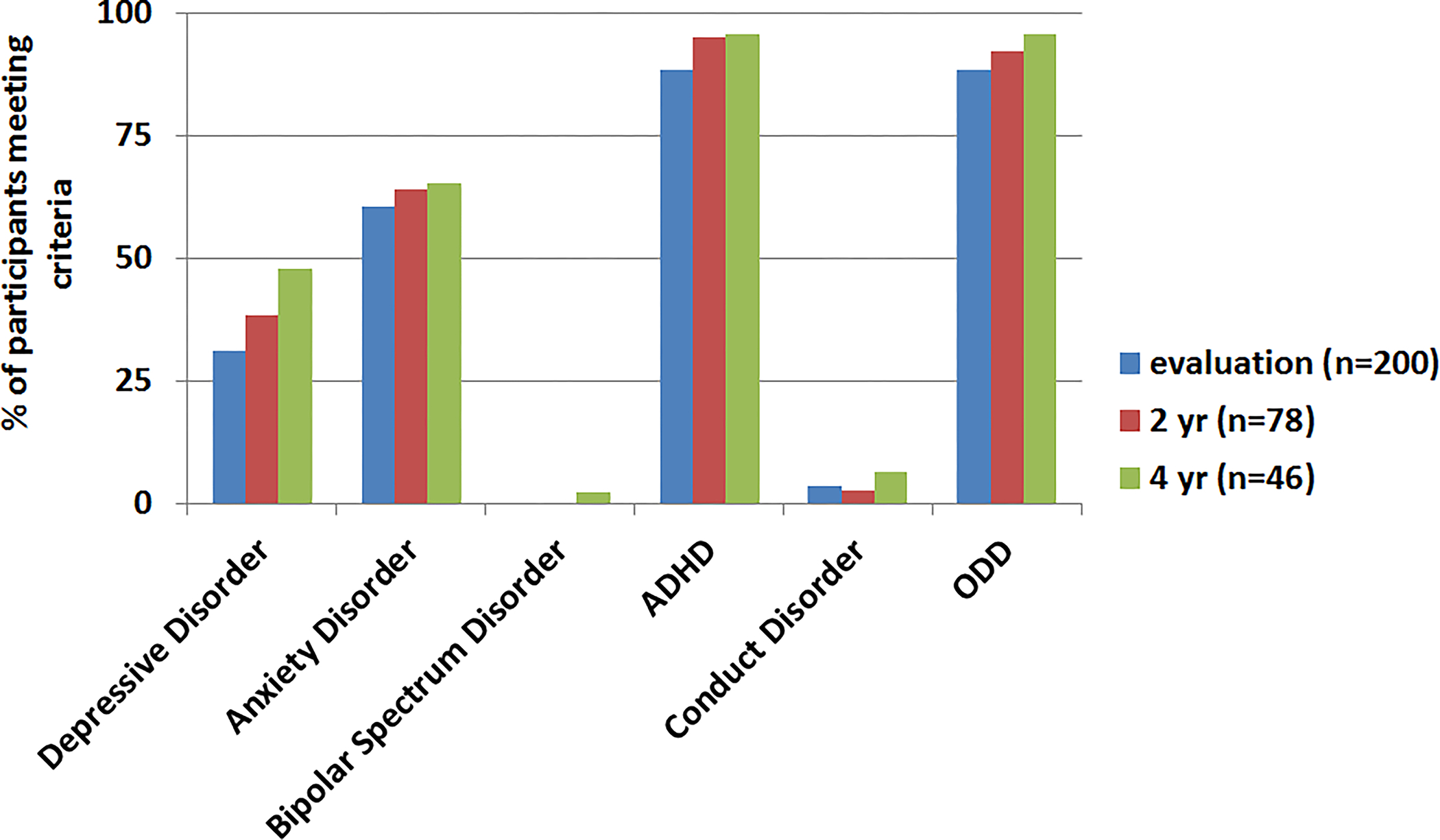
Methods: Youth meeting criteria for SMD (n = 200) were evaluated at baseline using standard diagnostic methods. Two-year (n = 78) and 4-year (n = 46) follow-up diagnostic and clinical impairment ratings collected at 6-month intervals were completed with those youths enrolled in the study for a sufficient time.
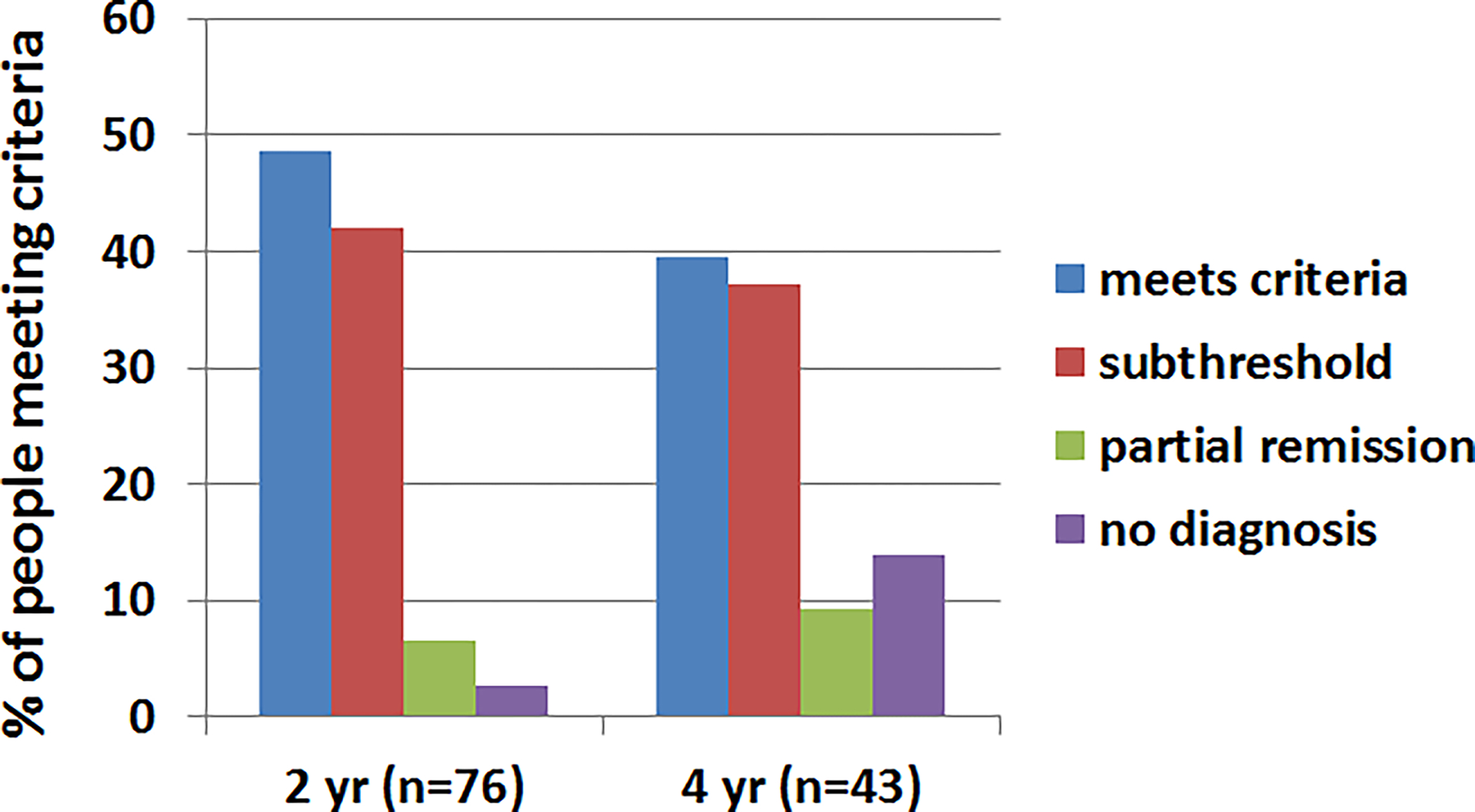
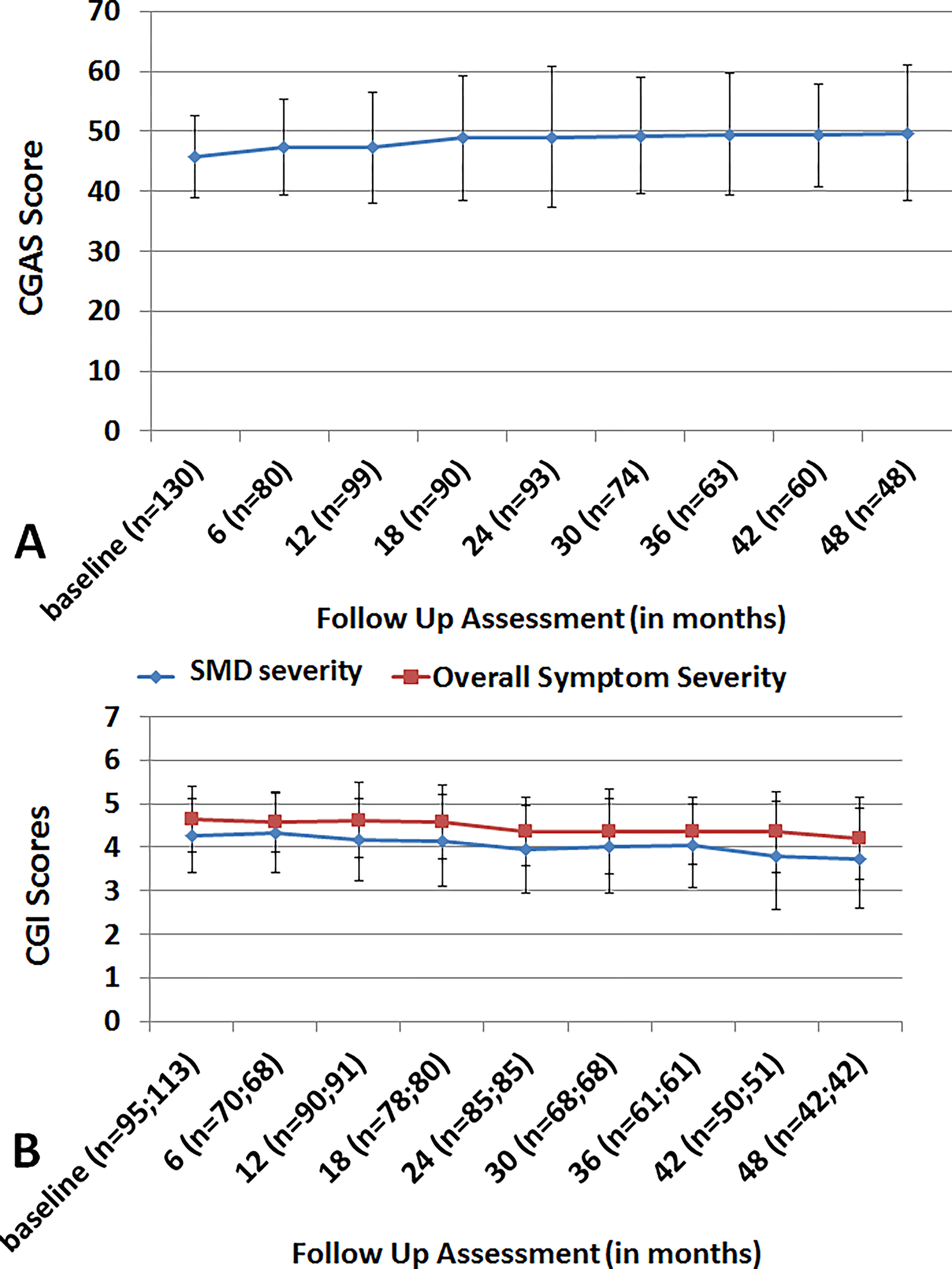
Results: Although the number of youth meeting strict categorical SMD criteria declined over time (49 and 40% at 2 and 4 years, respectively), many individuals not meeting full criteria continued to display clinically significant irritability symptoms (2 years: 42%; 4 years: 37%). Impairment due to these irritability symptoms remained consistently in the moderate range on the Clinical Global Impressions Scale.
Conclusions: By the 4-year follow-up, only 40% of youths meet strict SMD criteria; however, most continue to display clinically impairing symptoms and significant impairment warranting psychiatric treatment. These findings provide evidence for the course of irritability, with implications for DMDD. Future research with populations meeting DMDD criteria and followed through the ages of high risk for psychiatric diagnoses is necessary.
Trial registration: ClinicalTrials.gov NCT00025935.
Keywords: DMDD; irritability; longitudinal; severe mood dysregulation.
Published 2014. This article is a U.S. Government work and is in the public domain in the USA.
Figures

References
-
- Brotman MA, Schmajuk M, Rich BA, Dickstein DP, Guyer AE, Costello EJ, et al. Prevalence, clinical correlates, and longitudinal course of severe mood dysregulation in children. Biol Psychiatry. 2006;60(9):991–7. - PubMed
-
- Pickles A, Aglan A, Collishaw S, Messer J, Rutter M, Maughan B. Predictors of suicidality across the life span: the Isle of Wight study. Psychological medicine. 2010;40(9):1453–66. - PubMed
-
- Andreassi JL. Psychophysiology: Human behavior and psychophysiological response. 3rd ed. Hillsdale, N.J.: Erlbaum; 1995.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
