

MRI findings of radiation-associated angiosarcoma of the breast (RAS)
- PMID: 25504856
- PMCID: PMC4539138
- DOI: 10.1002/jmri.24822
MRI findings of radiation-associated angiosarcoma of the breast (RAS)
Abstract
Purpose: To describe the magnetic resonance imaging (MRI) characteristics of radiation-associated breast angiosarcomas (RAS).
Materials and methods: In this Institutional Review board (IRB)-approved retrospective study, 57 women were diagnosed with pathologically confirmed RAS during the study period (January 1999 to May 2013). Seventeen women underwent pretreatment breast MRI (prior to surgical resection or chemotherapy), of which 16 studies were available for review. Imaging features, including all available mammograms, ultrasounds, and breast MRIs, of these patients were evaluated by two radiologists independently and correlated with clinical management and outcomes.
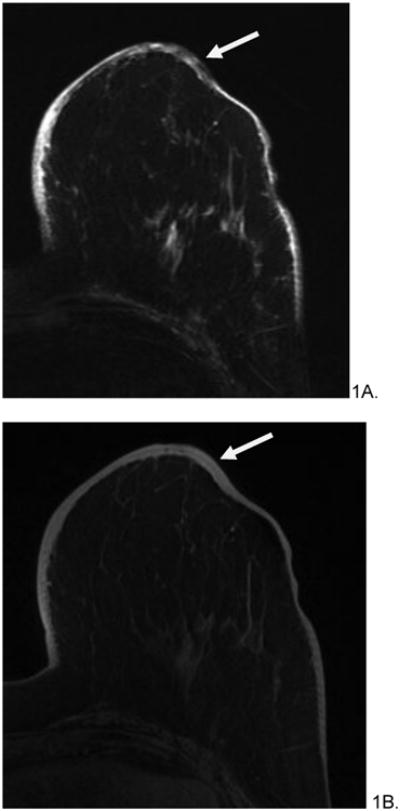
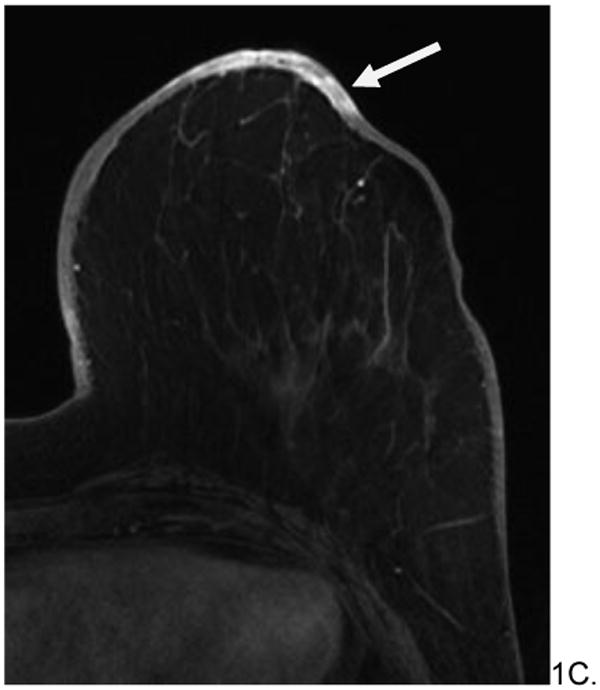
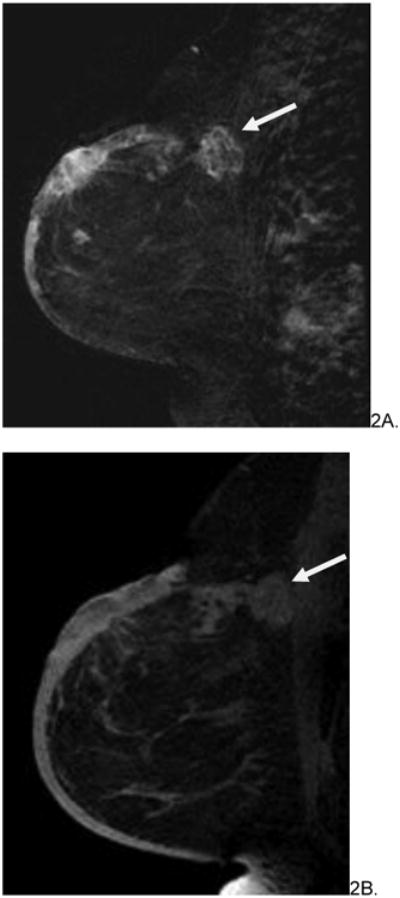
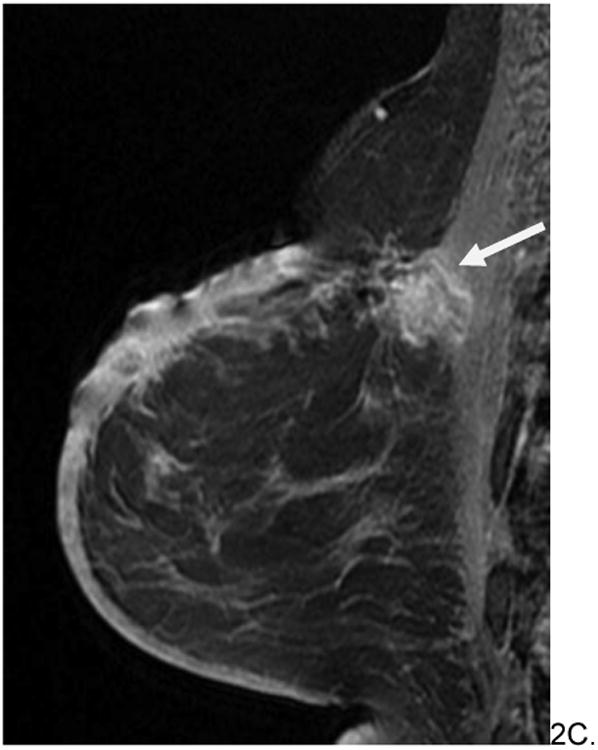
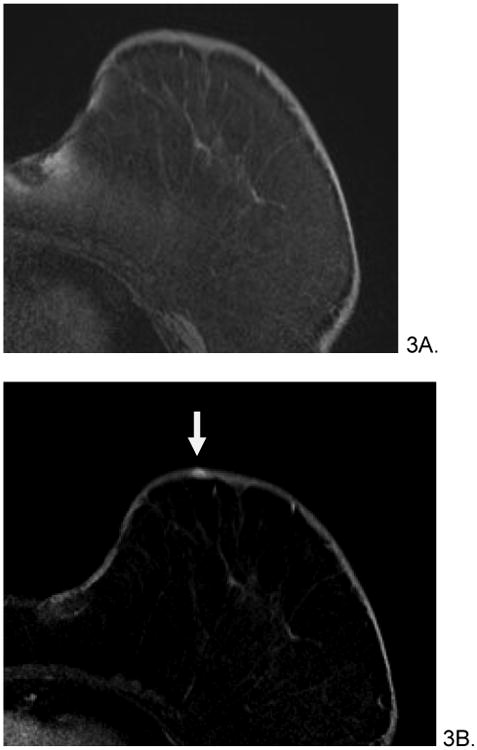
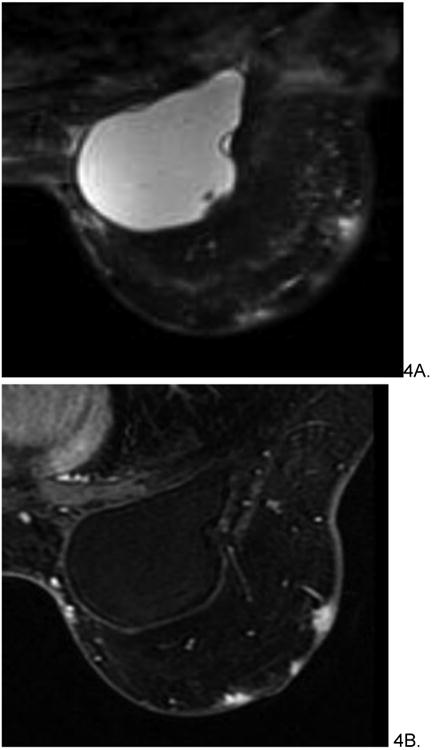
Results: The median age of patients at original breast cancer diagnosis was 69.3 years (range 42-84 years), with average time from initial radiation therapy to diagnosis of RAS of 7.3 years (range 5.1-9.5 years). Nine women had mammograms (9/16, 56%) and six had breast ultrasound (US) (6/16, 38%) prior to MRI, which demonstrated nonsuspicious findings in 5/9 mammograms and 3/6 ultrasounds. Four patients had distinct intraparenchymal masses on mammogram and MRI. MRI findings included diffuse T2 high signal skin thickening (16/16, 100%). Nearly half (7/16, 44%) of patients had T2 low signal intensity lesions; all lesions rapidly enhanced on postcontrast T1 -weighted imaging. All women underwent surgical resection, with 8/16 (50%) receiving neoadjuvant chemotherapy. Four women died during the study period.
Conclusion: Clinical, mammographic, and sonographic findings of RAS are nonspecific and may be occult on conventional breast imaging; MRI findings of RAS include rapidly enhancing dermal and intraparenchymal lesions, some of which are low signal on T2 weighted imaging.
Keywords: angiosarcoma; breast magnetic resonance imaging; radiation-associated.
© 2014 Wiley Periodicals, Inc.
Figures
References
-
- Huang J, Mackillop WJ. Increased risk of soft tissue sarcoma after radiotherapy in women with breast carcinoma. Cancer. 2001;92:172–180. - PubMed
-
- Glazebrook KN, Magut MJ, Reynolds C. Angiosarcoma of the breast. AJR American journal of roentgenology. 2008;190:533–538. - PubMed
-
- Cabete J, Lencastre A, Fidalgo A, Lobo L, Joao A, Serrao V. Postradiation cutaneous angiosarcoma of the breast: a diagnosis to keep in mind. The breast journal. 2014;20:89–90. - PubMed
-
- Morgan EA, Kozono DE, Wang Q, et al. Cutaneous radiation-associated angiosarcoma of the breast: poor prognosis in a rare secondary malignancy. Annals of surgical oncology. 2012;19:3801–3808. - PubMed
-
- Abbott R, Palmieri C. Angiosarcoma of the breast following surgery and radiotherapy for breast cancer. Nature clinical practice Oncology. 2008;5:727–736. - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
