

Virtual HDR CyberKnife SBRT for Localized Prostatic Carcinoma: 5-Year Disease-Free Survival and Toxicity Observations
- PMID: 25505732
- PMCID: PMC4241836
- DOI: 10.3389/fonc.2014.00321
Virtual HDR CyberKnife SBRT for Localized Prostatic Carcinoma: 5-Year Disease-Free Survival and Toxicity Observations
Abstract
Purpose: Prostate stereotactic body radiotherapy (SBRT) may substantially recapitulate the dose distribution of high-dose-rate (HDR) brachytherapy, representing an externally delivered "Virtual HDR" treatment method. Herein, we present 5-year outcomes from a cohort of consecutively treated virtual HDR SBRT prostate cancer patients.
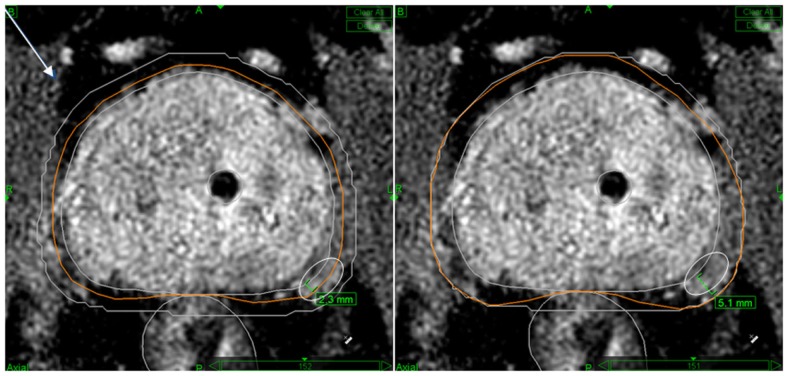
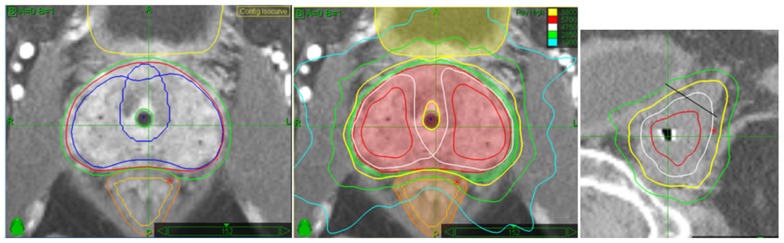
Methods: Seventy-nine patients were treated from 2006 to 2009, 40 low-risk, and 39 intermediate-risk, under IRB-approved clinical trial, to 38 Gy in four fractions. The planning target volume (PTV) included prostate plus a 2-mm volume expansion in all directions, with selective use of a 5-mm prostate-to-PTV expansion and proximal seminal vesicle coverage in intermediate-risk patients, to better cover potential extraprostatic disease; rectal PTV margin reduced to zero in all cases. The prescription dose covered >95% of the PTV (V100 ≥95%), with a minimum 150% PTV dose escalation to create "HDR-like" PTV dose distribution.
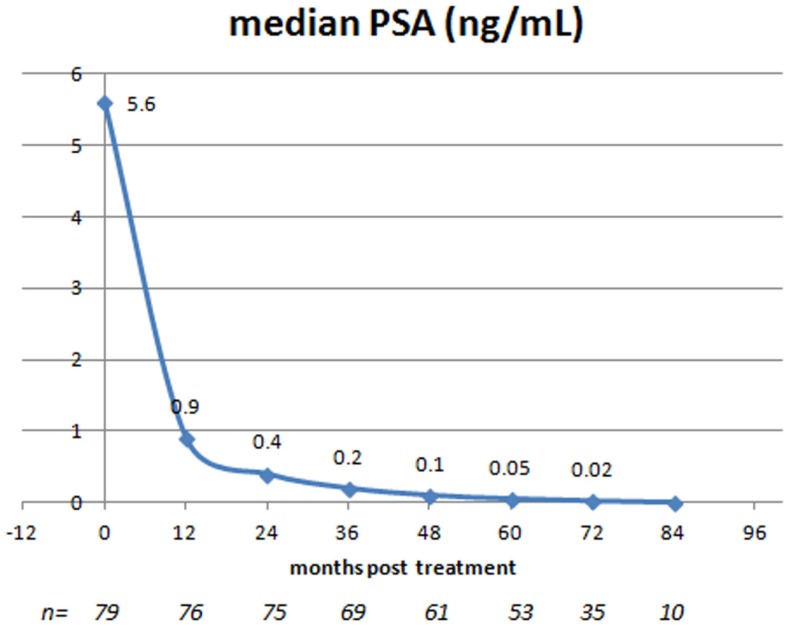
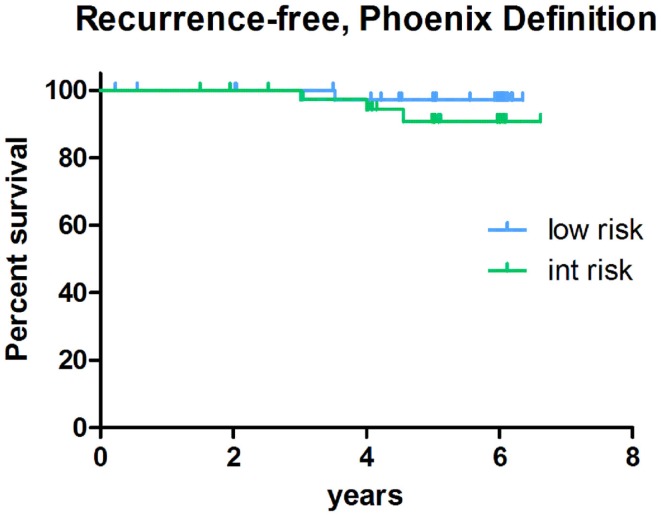
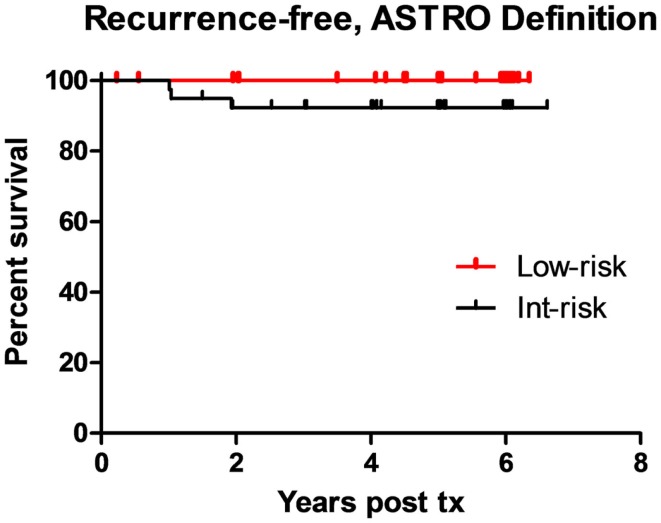
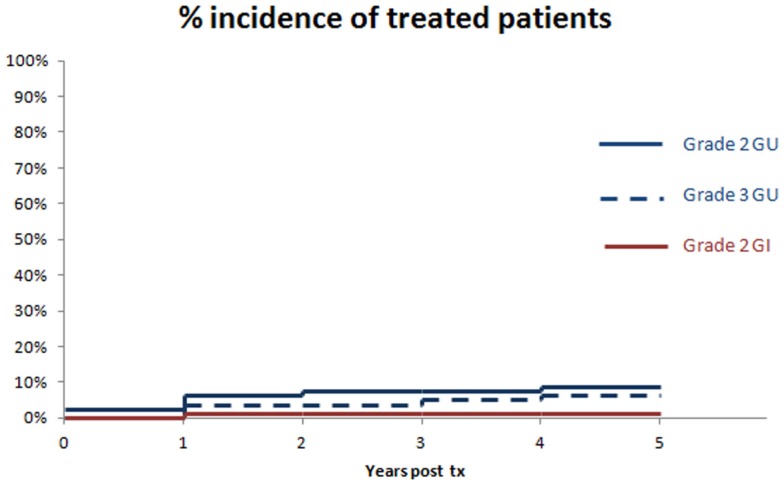
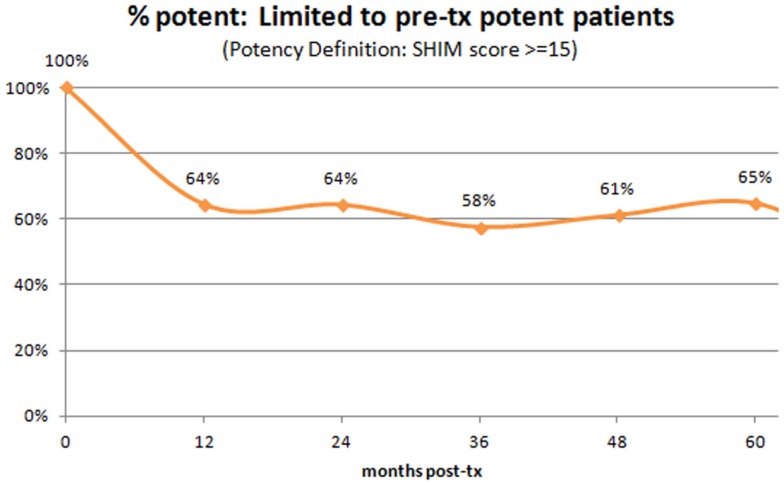
Results: Median pre-SBRT PSA level of 5.6 ng/mL decreased to 0.05 ng/mL 5 years out and 0.02 ng/mL 6 years out. At least one PSA bounce was seen in 55 patients (70%) but only 3 of them subsequently relapsed, biochemical-relapse-free survival was 100 and 92% for low-risk and intermediate-risk patients, respectively, by ASTRO definition (98 and 92% by Phoenix definition). Local relapse did not occur, distant metastasis-free survival was 100 and 95% by risk-group, and disease-specific survival was 100%. Acute and late grade 2 GU toxicity incidence was 10 and 9%, respectively; with 6% late grade 3 GU toxicity. Acute urinary retention did not occur. Acute and late grade 2 GI toxicity was 0 and 1%, respectively, with no grade 3 or higher toxicity. Of patient's potent pre-SBRT, 65% remained so at 5 years.
Conclusion: Virtual HDR prostate SBRT creates a very low PSA nadir, a high rate of 5-year disease-free survival and an acceptable toxicity incidence, with results closely resembling those reported post-HDR brachytherapy.
Keywords: CyberKnife; HDR; brachytherapy; dosimetry; image guided; prostate cancer; stereotactic body radiotherapy.
Figures
Similar articles
-
Early outcomes of high-dose-rate brachytherapy combined with ultra-hypofractionated radiation in higher-risk prostate cancer.Brachytherapy. 2021 Nov-Dec;20(6):1099-1106. doi: 10.1016/j.brachy.2021.08.006. Epub 2021 Sep 26. Brachytherapy. 2021. PMID: 34588146
-
Assessment of HDR brachytherapy-replicating prostate radiotherapy planning for tomotherapy, cyberknife and VMAT.Med Dosim. 2022 Spring;47(1):61-69. doi: 10.1016/j.meddos.2021.08.003. Epub 2021 Sep 20. Med Dosim. 2022. PMID: 34551879
-
Stereotactic body radiotherapy as monotherapy or post-external beam radiotherapy boost for prostate cancer: technique, early toxicity, and PSA response.Int J Radiat Oncol Biol Phys. 2012 Jan 1;82(1):228-34. doi: 10.1016/j.ijrobp.2010.10.026. Epub 2010 Dec 22. Int J Radiat Oncol Biol Phys. 2012. PMID: 21183287
-
Salvage Reirradiation Options for Locally Recurrent Prostate Cancer: A Systematic Review.Front Oncol. 2021 Sep 9;11:681448. doi: 10.3389/fonc.2021.681448. eCollection 2021. Front Oncol. 2021. PMID: 34568012 Free PMC article.
-
High-dose-rate intensity-modulated brachytherapy with external beam radiotherapy for prostate cancer: California endocurietherapy's 10-year results.Int J Radiat Oncol Biol Phys. 2005 Apr 1;61(5):1306-16. doi: 10.1016/j.ijrobp.2004.08.014. Int J Radiat Oncol Biol Phys. 2005. PMID: 15817332 Review.
Cited by
-
Treatment planning optimization with beam motion modeling for dynamic arc delivery of SBRT using Cyberknife with multileaf collimation.Med Phys. 2019 Dec;46(12):5421-5433. doi: 10.1002/mp.13848. Epub 2019 Oct 22. Med Phys. 2019. PMID: 31587322 Free PMC article.
-
Stereotactic Body Radiation Therapy for Localized Prostate Cancer: A Systematic Review and Meta-Analysis of Over 6,000 Patients Treated On Prospective Studies.Int J Radiat Oncol Biol Phys. 2019 Jul 15;104(4):778-789. doi: 10.1016/j.ijrobp.2019.03.051. Epub 2019 Apr 6. Int J Radiat Oncol Biol Phys. 2019. PMID: 30959121 Free PMC article.
-
Beam selection for stereotactic ablative radiotherapy using Cyberknife with multileaf collimation.Med Eng Phys. 2019 Feb;64:28-36. doi: 10.1016/j.medengphy.2018.12.011. Epub 2018 Dec 20. Med Eng Phys. 2019. PMID: 30579786 Free PMC article.
-
Hypofractionated Radiation Therapy for Localized Prostate Cancer: An ASTRO, ASCO, and AUA Evidence-Based Guideline.J Clin Oncol. 2018 Oct 11;36(34):JCO1801097. doi: 10.1200/JCO.18.01097. Online ahead of print. J Clin Oncol. 2018. PMID: 30307776 Free PMC article. No abstract available.
-
Stereotactic Radiation Therapy versus Brachytherapy: Relative Strengths of Two Highly Efficient Options for the Treatment of Localized Prostate Cancer.Cancers (Basel). 2022 Apr 29;14(9):2226. doi: 10.3390/cancers14092226. Cancers (Basel). 2022. PMID: 35565355 Free PMC article. Review.
References
-
- King CR, Collins S, Fuller D, Wang PC, Kupelian P, Steinberg M, et al. Health-related quality of life after stereotactic body radiation therapy for localized prostate cancer: results from a multi-institutional consortium of prospective trials. Int J Radiat Oncol Biol Phys (2013) 87(5):939–45.10.1016/j.ijrobp.2013.08.019 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous