

doi: 10.1155/2014/702613.
Epub 2014 Nov 19.
Necrotizing Soft Tissue Infection Occurring after Exposure to Mycobacterium marinum
Affiliations
- PMID: 25506004
- PMCID: PMC4254079
- DOI: 10.1155/2014/702613
Item in Clipboard
Necrotizing Soft Tissue Infection Occurring after Exposure to Mycobacterium marinum
Case Rep Infect Dis.
2014.
Abstract
Cutaneous infections caused by Mycobacterium marinum have been attributed to aquarium or fish exposure after a break in the skin barrier. In most instances, the upper limbs and fingers account for a majority of the infection sites. While previous cases of necrotizing soft tissue infections related to M. marinum have been documented, the importance of our presenting case is to illustrate the aggressive nature of M. marinum resulting in a persistent necrotizing soft tissue infection of a finger that required multiple aggressive wound debridements, followed by an amputation of the affected extremity, in order to hasten recovery.
Figures
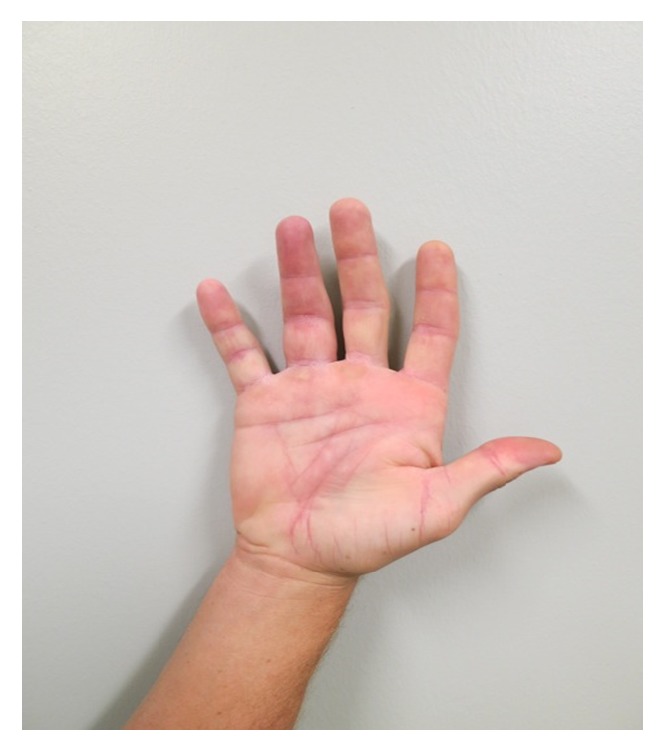
Initial presentation of injury. Three weeks after a barb fish spine penetrated the volar aspect of the proximal portion of his ring finger on his right hand. The injury occurred while fishing along one of the Charleston charters in August. He complained of a gradual increase in pain and swelling of the finger. On physical examination, entry and exit points were noted on the affected finger. Marked swelling was present; however, no bruising, cellulitis, discharge, erythema, or induration was noted. He was able to extend and flex the finger.

Tenosynovitis of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons. Clear nonpurulent fluid was noted around the tendons. A small puncture area was explored, and no foreign bodies were seen. Tissue samples were sent for pathology and routine and acid fast bacilli (AFB) cultures. Due to the high concern for a potential mycobacterial infection, clarithromycin, moxifloxacin, and rifabutin were started empirically. Three days later, he discontinued these medications due to gastrointestinal side effects from rifabutin without informing his physicians. Exudative cultures were negative; however, AFB cultures were positive, consistent with Mycobacterium marinum.
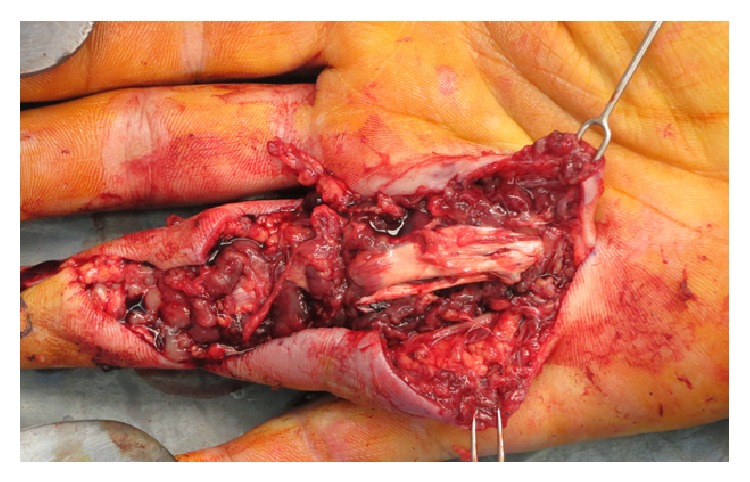
Debridement and radical synovectomy of his flexor tendon sheath secondary to necrotizing soft tissue infection. Erythema and induration surrounded the open wound, as well as nonviable wound edges that failed to bleed with manipulation, raising concern for a necrotizing soft tissue infection. He was immediately taken for surgical debridement and radical synovectomy of the right ring finger flexor tendon sheath, and tissue from the tendon sheath was sent for routine and mycobacterial cultures. Intravenous clarithromycin and moxifloxacin were initiated to empirically cover any potential superinfection. Twenty-four hours after admission, he was discharged to complete a six-month course of oral moxifloxacin and clarithromycin. AFB cultures were retuned positive, consistent with persistent Mycobacterium marinum.
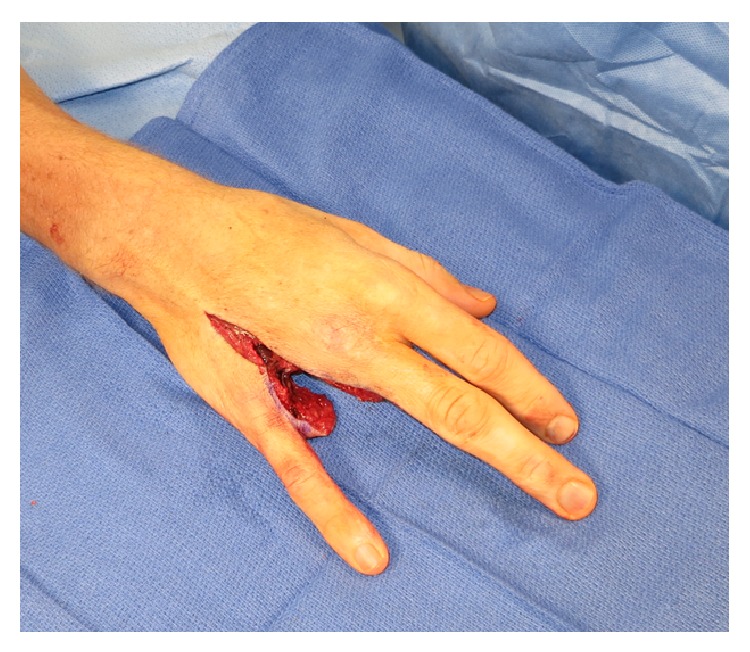
Persistent necrotizing soft tissue infection resulting in a ray amputation. Approximately one month following the second surgery, he presented to clinic with persistent swelling, erythema, induration, and dark necrotic appearing tissue along the base of the affected finger, consistent with persistent necrotizing soft tissue infection secondary to mycobacterial involvement. Ray amputation of the right ring finger was performed, and tissue pathology was consistent with granulomatous inflammation and necrosis, indicating a necrotizing soft tissue infection. Oral moxifloxacin and clarithromycin were continued to complete 6 months of therapy. During this time, he had marked clinical improvement and no evidence of persistent necrotizing soft tissue infection.
References
-
- Johnson R. P., Xia Y., Cho S., Burroughs R. F., Krivda S. J. Mycobacterium marinum infection: a case report and review of the literature. Cutis. 2007;79(1):33–36. - PubMed
-
- Dolenc-Voljc M., Zolnir-Dovc M. Delayed diagnosis of Mycobacterium marinum infection: a case report and review of the literature. Acta dermatovenerologica Alpina, Pannonica, et Adriatica. 2010;19(2):35–39. - PubMed
-
- Kumar A. R., Grewal N. S., Katchikian H. V., Jones N. F. Complex Mycobacterium marinum hand infections: case reports and review of literature. Infectious Diseases in Clinical Practice. 2008;16(5):278–282. doi: 10.1097/IPC.0b013e3181778886. - DOI
-
- Van Seymortier P., Verellen K., De Jonge I. Mycobacterium marinum causing tenosynovitis. ‘Fish tank finger’. Acta Orthopaedica Belgica. 2004;70(3):279–282. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
