

The use of semi-quantitative ultrasound elastosonography in combination with conventional ultrasonography and contrast-enhanced ultrasonography in the assessment of malignancy risk of thyroid nodules with indeterminate cytology
- PMID: 25506397
- PMCID: PMC4264546
- DOI: 10.1186/s13044-014-0009-8
The use of semi-quantitative ultrasound elastosonography in combination with conventional ultrasonography and contrast-enhanced ultrasonography in the assessment of malignancy risk of thyroid nodules with indeterminate cytology
Abstract
Background: The pre-surgical selection of thyroid nodules with indeterminate cytology (Thy 3 according to British Thyroid Association) after fine-needle aspiration biopsy (FNAB) is currently required in order to reduce unnecessary total thyroidectomy. The objective of our study was to use a surgical series of Thy 3 nodules to evaluate the predictive role of ultrasound elastosonography (USE) and contrast-enhanced ultrasonography (CEUS) in pre-surgical diagnoses of malignancy.
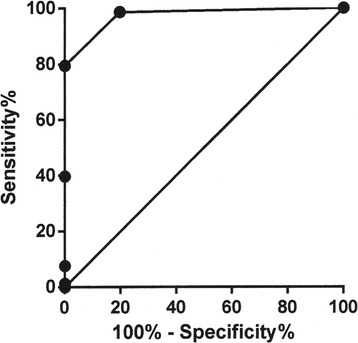
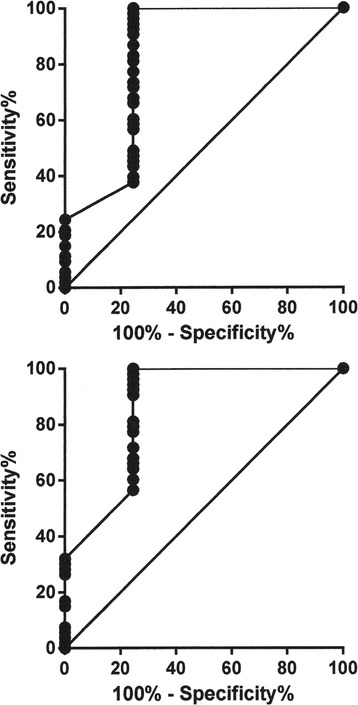
Subjects and methods: We enrolled 63 patients with Thy 3 nodules in which cytological-histological correlation was available. The ELX 2/1 strain index was obtained by means of semi-quantitative USE, which was performed before surgery in addition to conventional ultrasonography (US) and contrast-enhanced US (CEUS) on the Thy 3 nodules. The ELX 2/1 strain index, a five-item US score and both peak (P) index and time to peak (TTP) index from CEUS were correlated with the histological results. After surgical diagnosis, the data were analysed by using a receiver-operating characteristic (ROC) curve.
Results: Histology was benign in 50 and malignant in 13 Thy 3 nodules. No difference in maximal diameter was noted between benign (22.8 ± 1.6 mm) and malignant (18.9 ± 2.9 mm) nodules. Significant correlations were found between histology and cumulative US findings (p=0.005), ELX 2/1 index (p=0.002), P index (p=0.01) and TTP index (p=0.02). On analysing data from US, USE and CEUS, significant ROC areas under the curve were observed (p<0.0001). A cut-off value was set for US (>2), ELX 2/1 (>0.95), P index (<0.99) and TTP index (>0.98) scores. The diagnostic power of the cumulative pre-surgical analysis of Thy 3 nodules with US, USE and CEUS, considering the experimental cut-off points obtained from the ROC curves was: sensitivity 64%, specificity 92%, PPV 75% and accuracy 84%.
Conclusion: The ELX 2/1 index in conjunction with the US score can be useful in orienting surgical strategies in Thy 3 nodules. The information added by CEUS is less sensitive than that provided by US and USE. The use of a cut-off based on histology can reduce thyroidectomy. Observation should be the first choice when not all instrumental results are suspect.
Keywords: Contrast-enhanced ultrasonography; Cytological–histological correlation; Indeterminate cytology; ROC analysis; Strain index; Thyroid nodules; Ultrasosonography; Ultrasound elastosonography.
Figures

References
-
- Van der Bruel A, Francart J, Dubois C, Adam A, Vlayen J, De Schutter H, Stordeur S, Decallonne B. Regional variation in thyroid cancer incidence in Belgium is associated with variation in thyroid imaging and thyroid disease management. J Clin Endocrinol Metab. 2013;98:4063–4071. doi: 10.1210/jc.2013-1705. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
