

Successful treatment of infectious endocarditis associated glomerulonephritis mimicking c3 glomerulonephritis in a case with no previous cardiac disease
- PMID: 25506445
- PMCID: PMC4259083
- DOI: 10.1155/2014/569047
Successful treatment of infectious endocarditis associated glomerulonephritis mimicking c3 glomerulonephritis in a case with no previous cardiac disease
Abstract
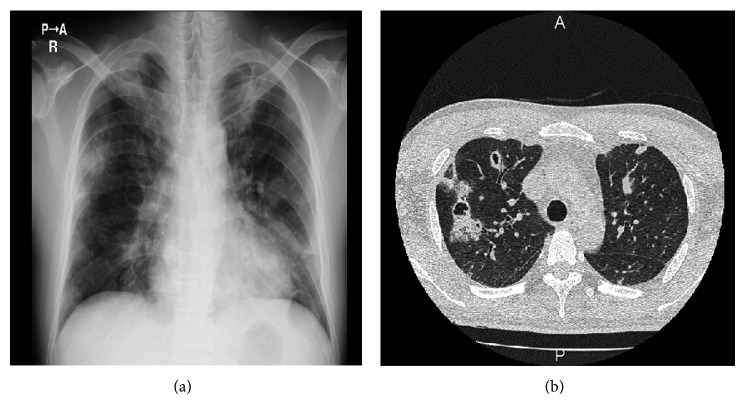
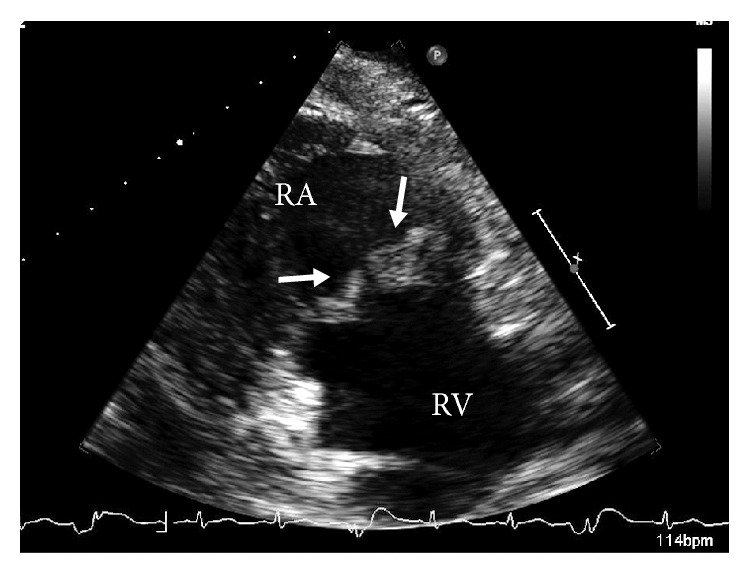
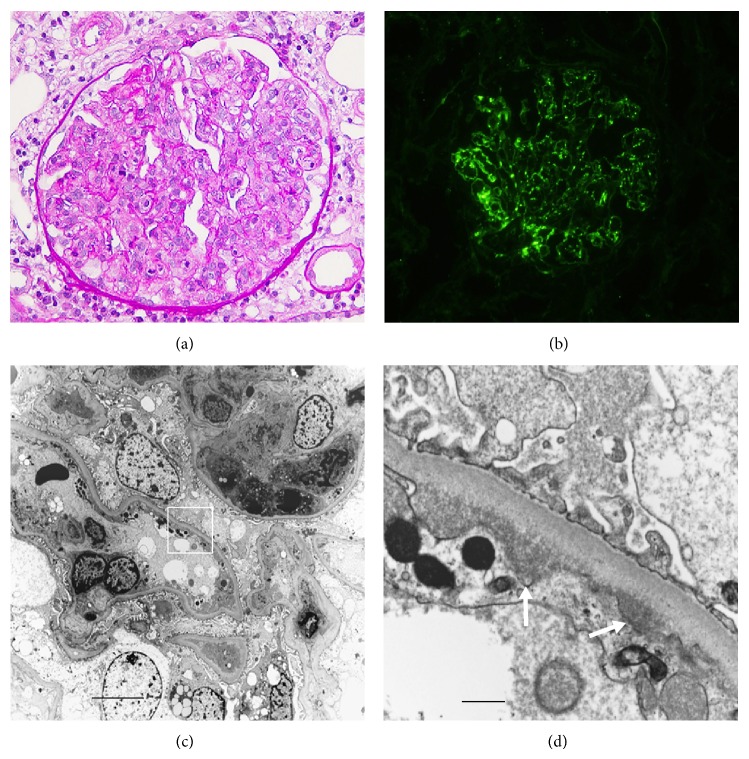
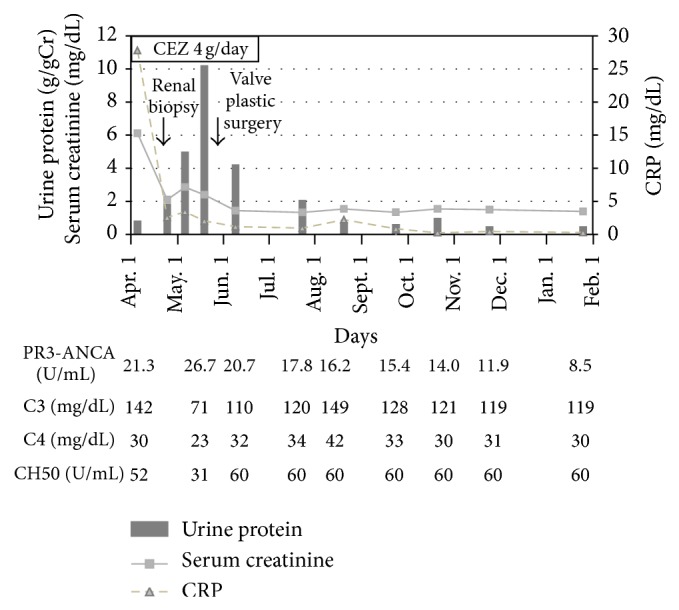
We report a 42-year-old man with subacute infectious endocarditis (IE) with septic pulmonary embolism, presenting rapidly progressive glomerulonephritis and positive proteinase 3-anti-neutrophil cytoplasmic antibody (PR3-ANCA). He had no previous history of heart disease. Renal histology revealed diffuse endocapillary proliferative glomerulonephritis with complement 3- (C3-) dominant staining and subendothelial electron dense deposit, mimicking C3 glomerulonephritis. Successful treatment of IE with valve plastic surgery gradually ameliorated hypocomplementemia and renal failure; thus C3 glomerulonephritis-like lesion in this case was classified as postinfectious glomerulonephritis. IE associated glomerulonephritis is relatively rare, especially in cases with no previous history of valvular disease of the heart like our case. This case also reemphasizes the broad differential diagnosis of renal involvement in IE.
Figures
Similar articles
-
Diagnostic and treatment challenge of unrecognized subacute bacterial endocarditis associated with ANCA-PR3 positive immunocomplex glomerulonephritis: a case report and literature review.BMC Nephrol. 2020 Jan 31;21(1):40. doi: 10.1186/s12882-020-1694-2. BMC Nephrol. 2020. PMID: 32005179 Free PMC article. Review.
-
PR3-ANCA-positive crescentic necrotizing glomerulonephritis accompanied by isolated pulmonic valve infective endocarditis, with reference to previous reports of renal pathology.Clin Nephrol. 2006 Sep;66(3):202-9. doi: 10.5414/cnp66202. Clin Nephrol. 2006. PMID: 16995343
-
Endocarditis-Associated C3-Dominant Glomerulonephritis in a Patient With a Solitary Kidney.Cureus. 2022 Aug 4;14(8):e27675. doi: 10.7759/cureus.27675. eCollection 2022 Aug. Cureus. 2022. PMID: 35935112 Free PMC article.
-
Cytoplasmic antineutrophil cytoplasmic antibody positive pauci-immune glomerulonephritis associated with infectious endocarditis.Clin Nephrol. 2006 Dec;66(6):447-54. doi: 10.5414/cnp66447. Clin Nephrol. 2006. PMID: 17176917
-
Bartonella henselae endocarditis and glomerulonephritis with dominant C3 deposition in a 21-year-old male with a Melody transcatheter pulmonary valve: case report and review of the literature.Pediatr Dev Pathol. 2014 Jul-Aug;17(4):312-20. doi: 10.2350/14-04-1462-CR.1. Epub 2014 Jun 4. Pediatr Dev Pathol. 2014. PMID: 24896298 Review.
Cited by
-
Antineutrophil cytoplasmic antibody-positive infective endocarditis complicated by acute kidney injury: a case report and literature review.J Int Med Res. 2020 Oct;48(10):300060520963990. doi: 10.1177/0300060520963990. J Int Med Res. 2020. PMID: 33078666 Free PMC article. Review.
-
Vasculitides and glomerulonephritis associated with Staphylocococcus aureus infective endocarditis: cases reports and mini-review of the literature.Ann Med. 2020 Sep;52(6):265-274. doi: 10.1080/07853890.2020.1778778. Epub 2020 Jun 26. Ann Med. 2020. PMID: 32588668 Free PMC article. Review.
-
Proteinase 3-antineutrophil cytoplasmic antibody-positive necrotizing crescentic glomerulonephritis complicated by infectious endocarditis: a case report.J Med Case Rep. 2019 Dec 5;13(1):356. doi: 10.1186/s13256-019-2287-1. J Med Case Rep. 2019. PMID: 31801609 Free PMC article.
-
Antineutrophil Cytoplasmic Antibodies Associated With Infective Endocarditis.Medicine (Baltimore). 2016 Jan;95(3):e2564. doi: 10.1097/MD.0000000000002564. Medicine (Baltimore). 2016. PMID: 26817911 Free PMC article.
-
Antineutrophil Cytoplasmic Antibody Induction due to Infection: A Patient with Infective Endocarditis and Chronic Hepatitis C.Can J Infect Dis Med Microbiol. 2016;2016:3585860. doi: 10.1155/2016/3585860. Epub 2016 Mar 21. Can J Infect Dis Med Microbiol. 2016. PMID: 27366166 Free PMC article.
References
-
- Peng H., Chen W.-F., Wu C., Chen Y.-R., Peng B., Paudel S. D., Lou T.-Q. Culture-negative subacute bacterial endocarditis masquerades as granulomatosis with polyangiitis (Wegener's granulomatosis) involving both the kidney and lung. BMC Nephrology. 2012;13, article 174 doi: 10.1186/1471-2369-13-174. - DOI - PMC - PubMed
-
- Sethi S., Fervenza F. C., Zhang Y., Zand L., Meyer N. C., Borsa N., Nasr S. H., Smith R. J. H. Atypical postinfectious glomerulonephritis is associated with abnormalities in the alternative pathway of complement. Kidney International. 2013;83(2):293–299. doi: 10.1038/ki.2012.384. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
