

Pancreatic cancer metastasis: are we being pre-EMTed?
- PMID: 25506899
- PMCID: PMC4457289
- DOI: 10.2174/1381612821666141211115234
Pancreatic cancer metastasis: are we being pre-EMTed?
Abstract
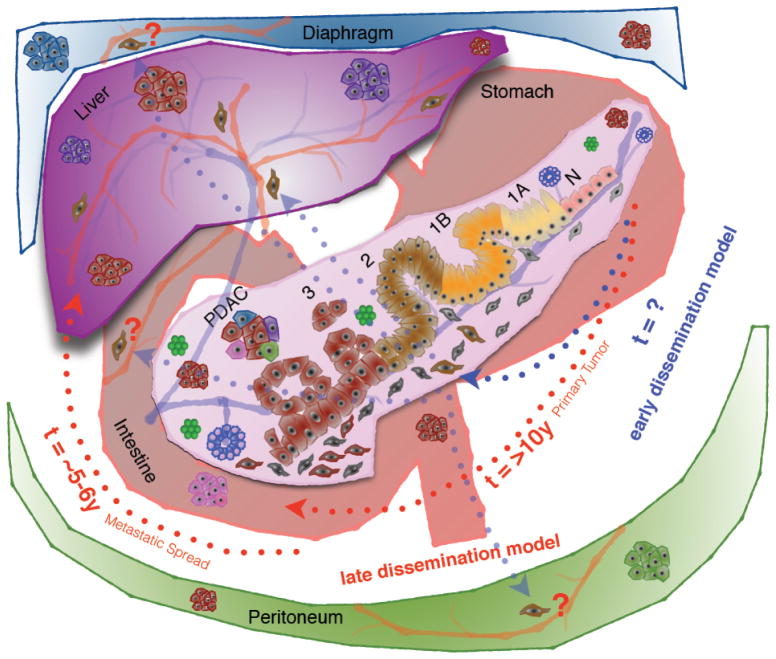
Pancreatic cancer, often considered a metastatic disease at the time of clinical diagnosis due to lack of any reliable early diagnostic marker(s), is refractory to conventional chemo- and radiotherapy and has a dismal 5-year survival rate of only 6%. Although surgical removal of the primary tumor is considered to be curative, the 5-year survival rate is no more than 20% even in patients with clear resection margins (R0). The recurrence of local and metastatic disease (primarily liver metastasis) post resection is considered to be the leading cause of mortality in these patients. In addition, instances of metastatic disease without any local recurrence post resection have also been observed. Cancer metastasis is the primary cause of mortality in cancer patients and is classically viewed as a late event during the progression of the disease, which is supported by the genetic studies used to understand the evolution of pancreatic cancer. However, this view has recently been challenged by studies using mathematical modeling and genetically labeled mouse models of pancreatic cancer to understand the dynamics of tumor cell dissemination and epithelial to mesenchymal transition (EMT) of tumor cells well before the primary tumor is formed. Given that EMT is a hallmark process that initiates the metastatic seeding of cancer cells and the dismal prognosis of pancreatic cancer patients even after efficient removal of the primary tumor (99.9%), an early dissemination hypothesis of cancer cells cannot be undermined. In this review, we will discuss the current views regarding pancreatic cancer metastasis with particular emphasis on the epithelial to mesenchymal transition, its influence on the selection of patients for surgical resection and the therapeutic intervention.
Conflict of interest statement
The authors confirm that this article content has no conflict of interest.
Figures
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64:9–29. - PubMed
-
- Konstantinidis IT, Warshaw AL, Allen JN, et al. Pancreatic ductal adenocarcinoma: is there a survival difference for R1 resections versus locally advanced unresectable tumors? What is a “true” R0 resection? Ann Surg. 2013;257:731–6. - PubMed
-
- Richter A, Niedergethmann M, Sturm JW, et al. Long-term results of partial pancreaticoduodenectomy for ductal adenocarcinoma of the pancreatic head: 25-year experience. World J Surg. 2003;27:324–9. - PubMed
-
- La Torre M, Nigri G, Ferrari L, et al. Hospital volume, margin status, and long-term survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. Am Surg. 2012;78:225–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical