

Rapid generation of clinical-grade antiviral T cells: selection of suitable T-cell donors and GMP-compliant manufacturing of antiviral T cells
- PMID: 25510656
- PMCID: PMC4335407
- DOI: 10.1186/s12967-014-0336-5
Rapid generation of clinical-grade antiviral T cells: selection of suitable T-cell donors and GMP-compliant manufacturing of antiviral T cells
Abstract
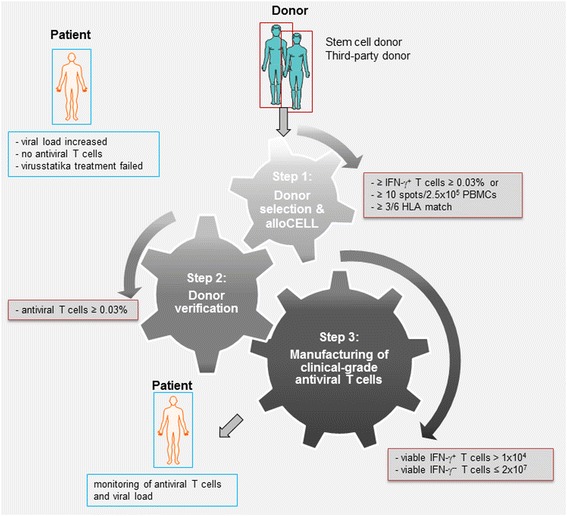
Background: The adoptive transfer of allogeneic antiviral T lymphocytes derived from seropositive donors can safely and effectively reduce or prevent the clinical manifestation of viral infections or reactivations in immunocompromised recipients after hematopoietic stem cell (HSCT) or solid organ transplantation (SOT). Allogeneic third party T-cell donors offer an alternative option for patients receiving an allogeneic cord blood transplant or a transplant from a virus-seronegative donor and since donor blood is generally not available for solid organ recipients. Therefore we established a registry of potential third-party T-cell donors (allogeneic cell registry, alloCELL) providing detailed data on the assessment of a specific individual memory T-cell repertoire in response to antigens of cytomegalovirus (CMV), Epstein-Barr virus (EBV), adenovirus (ADV), and human herpesvirus (HHV) 6.
Methods: To obtain a manufacturing license according to the German Medicinal Products Act, the enrichment of clinical-grade CMV-specific T cells from three healthy CMV-seropositive donors was performed aseptically under GMP conditions using the CliniMACS cytokine capture system (CCS) after restimulation with an overlapping peptide pool of the immunodominant CMVpp65 antigen. Potential T-cell donors were selected from alloCELL and defined as eligible for clinical-grade antiviral T-cell generation if the peripheral fraction of IFN-γ(+) T cells exceeded 0.03% of CD3(+) lymphocytes as determined by IFN-γ cytokine secretion assay.
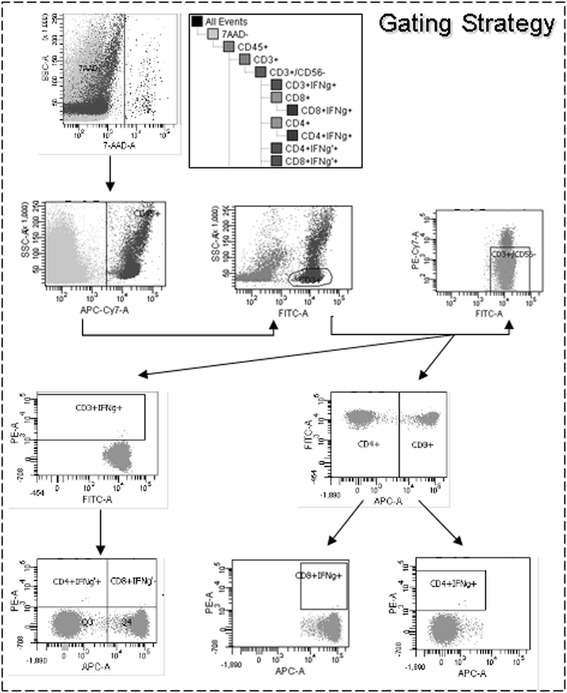
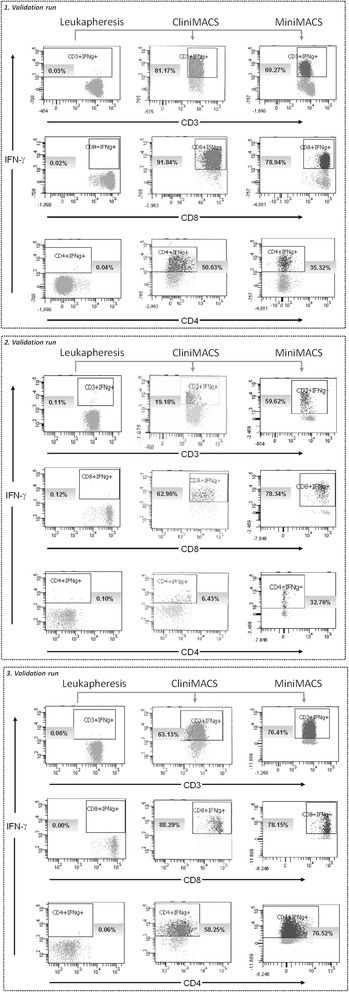
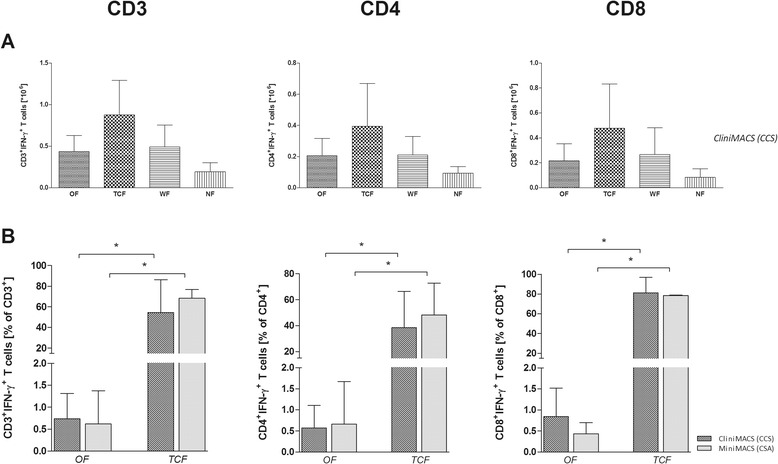
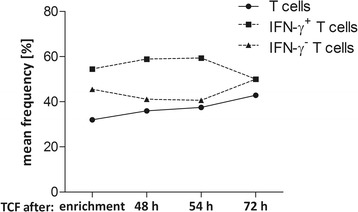
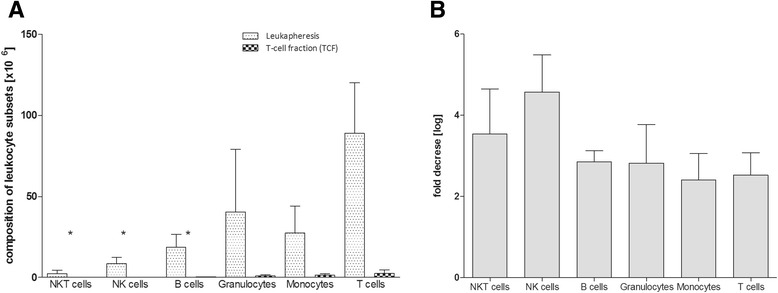
Results: Starting with low concentration of IFN-γ(+) T cells (0.07-1.11%) we achieved 81.2%, 19.2%, and 63.1% IFN-γ(+)CD3(+) T cells (1.42 × 10(6), 0.05 × 10(6), and 1.15 × 10(6)) after enrichment. Using the CMVpp65 peptide pool for restimulation resulted in the activation of more CMV-specific CD8(+) than CD4(+) memory T cells, both of which were effectively enriched to a total of 81.0% CD8(+)IFN-γ(+) and 38.4% CD4(+)IFN-γ(+) T cells. In addition to T cells and NKT cells, all preparations contained acceptably low percentages of contaminating B cells, granulocytes, monocytes, and NK cells. The enriched T-cell products were stable over 72 h with respect to viability and ratio of T lymphocytes.
Conclusions: The generation of antiviral CD4(+) and CD8(+) T cells by CliniMACS CCS can be extended to a broad spectrum of common pathogen-derived peptide pools in single or multiple applications to facilitate and enhance the efficacy of adoptive T-cell immunotherapy.
Figures
References
-
- Aissi-Rothe L, Decot V, Venard V, Jeulin H, Salmon A, Clement L, Kennel A, Mathieu C, Dalle JH, Rauser G, Cambouris C, de Carvalho M, Stoltz JF, Bordigoni P, Bensoussan D. Rapid generation of full clinical-grade human antiadenovirus cytotoxic T cells for adoptive immunotherapy. J Immunother. 2010;33:414–424. doi: 10.1097/CJI.0b013e3181cc263b. - DOI - PubMed
-
- Doubrovina E, Oflaz-Sozmen B, Prockop SE, Kernan NA, Abramson S, Teruya-Feldstein J, Hedvat C, Chou JF, Heller G, Barker JN, Boulad F, Castro-Malaspina H, George D, Jakubowski A, Koehne G, Papadopoulos EB, Scaradavou A, Small TN, Khalaf R, Young JW, O'Reilly RJ. Adoptive immunotherapy with unselected or EBV-specific T cells for biopsy-proven EBV+ lymphomas after allogeneic hematopoietic cell transplantation. Blood. 2012;119:2644–2656. doi: 10.1182/blood-2011-08-371971. - DOI - PMC - PubMed
-
- Feuchtinger T, Opherk K, Bethge WA, Topp MS, Schuster FR, Weissinger EM, Mohty M, Or R, Maschan M, Schumm M, Hamprecht K, Handgretinger R, Lang P, Einsele H. Adoptive transfer of pp 65-specific T cells for the treatment of chemorefractory cytomegalovirus disease or reactivation after haploidentical and matched unrelated stem cell transplantation. Blood. 2010;116:4360–4367. doi: 10.1182/blood-2010-01-262089. - DOI - PubMed
-
- Feuchtinger T, Richard C, Joachim S, Scheible MH, Schumm M, Hamprecht K, Martin D, Jahn G, Handgretinger R, Lang P. Clinical grade generation of hexon-specific T cells for adoptive T-cell transfer as a treatment of adenovirus infection after allogeneic stem cell transplantation. J Immunother. 2008;31:199–206. doi: 10.1097/CJI.0b013e31815ef862. - DOI - PubMed
-
- Heslop HE, Slobod KS, Pule MA, Hale GA, Rousseau A, Smith CA, Bollard CM, Liu H, Wu MF, Rochester RJ, Amrolia PJ, Hurwitz JL, Brenner MK, Rooney CM. Long-term outcome of EBV-specific T-cell infusions to prevent or treat EBV-related lymphoproliferative disease in transplant recipients. Blood. 2010;115:925–935. doi: 10.1182/blood-2009-08-239186. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
