

Comparative genomic profiling of synovium versus skin lesions in psoriatic arthritis
- PMID: 25512250
- PMCID: PMC4406155
- DOI: 10.1002/art.38995
Comparative genomic profiling of synovium versus skin lesions in psoriatic arthritis
Abstract
Objective: To our knowledge, there is no broad genomic analysis comparing skin and synovium in psoriatic arthritis (PsA). Also, there is little understanding of the relative levels of cytokines and chemokines in skin and synovium. The purpose of this study was to better define inflammatory pathways in paired lesional skin and affected synovial tissue in patients with PsA.
Methods: We conducted a comprehensive analysis of cytokine and chemokine activation and genes representative of the inflammatory processes in PsA. Paired PsA synovial tissue and skin samples were obtained from 12 patients on the same day. Gene expression studies were performed using Affymetrix HGU133 Plus 2.0 arrays. Confirmatory quantitative real-time polymerase chain reaction (PCR) was performed on selected transcripts. Cell populations were assessed by immunohistochemistry and immunofluorescence.
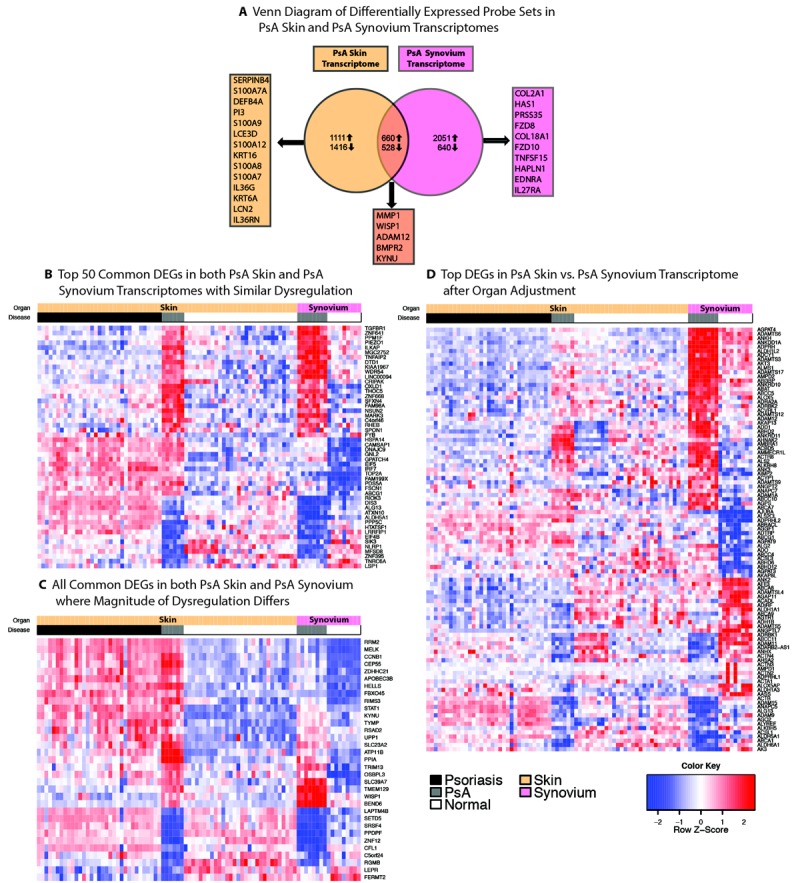
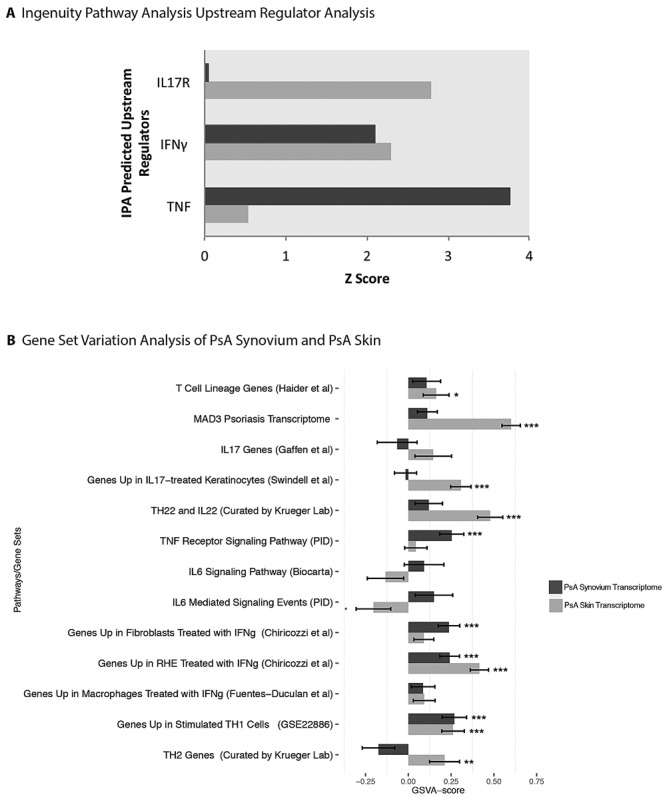
Results: Globally, gene expression in PsA synovium was more closely related to gene expression in PsA skin than to gene expression in synovium in other forms of arthritis. However, PsA gene expression patterns in skin and synovium were clearly distinct, showing a stronger interleukin-17 (IL-17) gene signature in skin than in synovium and more equivalent tumor necrosis factor (TNF) and interferon-γ gene signatures in both tissues. These results were confirmed with real-time PCR.
Conclusion: This is the first comprehensive molecular comparison of paired lesional skin and affected synovial tissue samples in PsA. Our results support clinical trial data showing that PsA skin and joint disease are similarly responsive to TNF antagonists, while IL-17 antagonists have better results in PsA skin than in PsA joints. Genes selectively expressed in PsA synovium might direct future therapies for PsA.
© 2015 The Authors. Arthritis & Rheumatology is published by Wiley Periodicals, Inc. on behalf of the American College of Rheumatology.
Figures


Comment in
-
Why did IL-23p19 inhibition fail in AS: a tale of tissues, trials or translation?Ann Rheum Dis. 2019 Aug;78(8):1015-1018. doi: 10.1136/annrheumdis-2018-213654. Epub 2018 Oct 8. Ann Rheum Dis. 2019. PMID: 30297330 Free PMC article. No abstract available.
References
-
- Zachariae H. Prevalence of joint disease in patients with psoriasis: implications for therapy. Am J Clin Dermatol. 2003;4:441–7. - PubMed
-
- Cauli A, Mathieu A. Th17 and interleukin 23 in the pathogenesis of psoriatic arthritis and spondyloarthritis. J Rheumatol. 2012;89(Suppl):15–8. - PubMed
-
- Chiricozzi A, Guttman-Yassky E, Suarez-Farinas M, Nograles KE, Tian S, Cardinale I. Integrative responses to IL-17 and TNF-α in human keratinocytes account for key inflammatory pathogenic circuits in psoriasis. J Invest Dermatol. 2011;131:677–87. - PubMed
-
- Jandus C, Bioley G, Rivals JP, Dudler J, Speiser D, Romero P. Increased numbers of circulating polyfunctional Th17 memory cells in patients with seronegative spondylarthritides. Arthritis Rheum. 2008;58:2307–17. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
