

Association of fluid overload with cardiovascular morbidity and all-cause mortality in stages 4 and 5 CKD
- PMID: 25512646
- PMCID: PMC4284411
- DOI: 10.2215/CJN.03610414
Association of fluid overload with cardiovascular morbidity and all-cause mortality in stages 4 and 5 CKD
Abstract
Background and objectives: Fluid overload is a common characteristic associated with renal progression in CKD. Additionally, fluid overload is an independent predictor of all-cause or cardiovascular mortality in patients on dialysis, but its influence on patients not on dialysis is uncertain. The aim of the study was to assess the relationship between the severity of fluid status and clinical outcomes in an advanced CKD cohort.
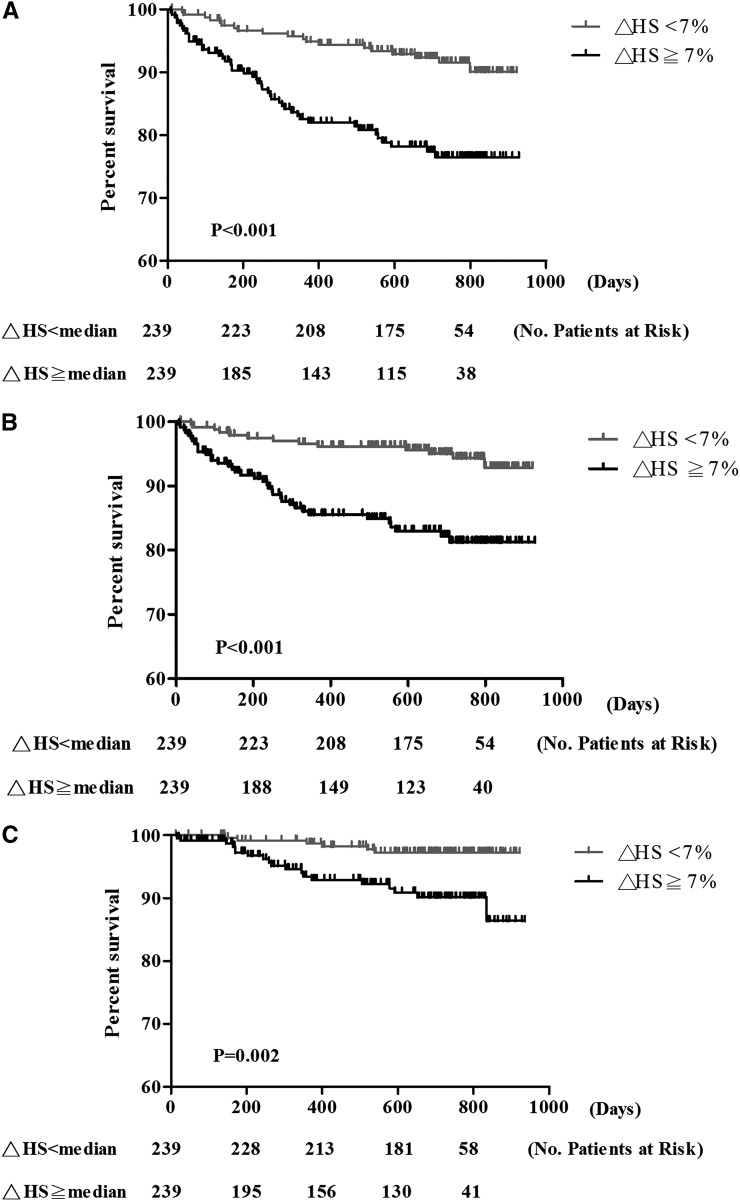
Design, setting, participants, & measurements: In total, 478 predialysis patients with stages 4 and 5 CKD in the integrated CKD care program were enrolled from January of 2011 to December of 2011 and followed-up until August of 2013. The clinical outcomes included cardiovascular morbidity and all-cause mortality. The relative hydration status (overhydration/extracellular water) was used as the presentation of the severity of fluid status and measured using a body composition monitor. Overhydration/extracellular water >7% was defined as fluid overload.
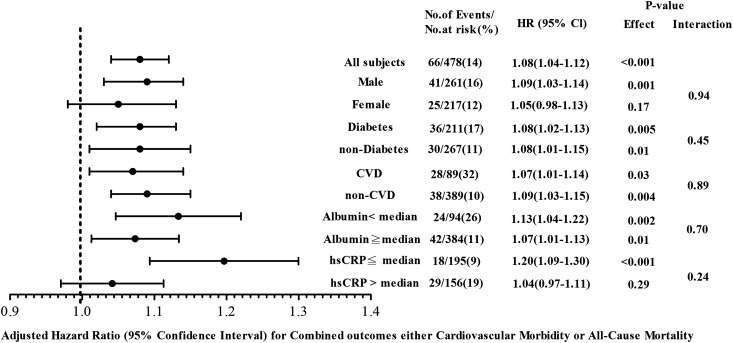
Results: Over a median follow-up period of 23.2 (12.6-26.4) months, 66 (13.8%) patients reached all-cause mortality or cardiovascular morbidity. The adjusted hazard ratio of the combined outcome of all-cause mortality or cardiovascular morbidity for every 1% higher overhydration/extracellular water was 1.08 (95% confidence interval, 1.04 to 1.12; P<0.001). The adjusted overhydration/extracellular water for the combined outcome of all-cause mortality or cardiovascular morbidity in participants with overhydration/extracellular water ≥7% compared with those with overhydration/extracellular water <7% was 1.93 (95% confidence interval, 1.01 to 3.69; P=0.04). In subgroup analysis, higher overhydration/extracellular water was consistently associated with increased risk for the combined outcome independent of diabetes, cardiovascular disease, and serum albumin. There was no significant interaction between all subgroups.
Conclusions: These findings suggest that fluid overload is an independent risk factor of the combined outcome of all-cause mortality or cardiovascular morbidity in patients with advanced CKD.
Keywords: CKD; cardiovascular disease; mortality.
Copyright © 2015 by the American Society of Nephrology.
Figures
Comment in
-
Is fluid overload as measured by bioimpedance spectroscopy harmful in CKD-if so, why?Clin J Am Soc Nephrol. 2015 Jan 7;10(1):1-3. doi: 10.2215/CJN.11311114. Epub 2014 Dec 15. Clin J Am Soc Nephrol. 2015. PMID: 25512645 Free PMC article. No abstract available.
References
-
- Meguid El Nahas A, Bello AK: Chronic kidney disease: The global challenge. Lancet 365: 331–340, 2005 - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Wizemann V, Leibinger A, Mueller K, Nilson A: Influence of hydration state on plasma volume changes during ultrafiltration. Artif Organs 19: 416–419, 1995 - PubMed
-
- Wizemann V, Schilling M: Dilemma of assessing volume state—the use and the limitations of a clinical score. Nephrol Dial Transplant 10: 2114–2117, 1995 - PubMed
-
- Paniagua R, Ventura MD, Avila-Díaz M, Hinojosa-Heredia H, Méndez-Durán A, Cueto-Manzano A, Cisneros A, Ramos A, Madonia-Juseino C, Belio-Caro F, García-Contreras F, Trinidad-Ramos P, Vázquez R, Ilabaca B, Alcántara G, Amato D: NT-proBNP, fluid volume overload and dialysis modality are independent predictors of mortality in ESRD patients. Nephrol Dial Transplant 25: 551–557, 2010 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
