

Effect of lung-protective ventilation with lower tidal volumes on clinical outcomes among patients undergoing surgery: a meta-analysis of randomized controlled trials
- PMID: 25512653
- PMCID: PMC4330165
- DOI: 10.1503/cmaj.141005
Effect of lung-protective ventilation with lower tidal volumes on clinical outcomes among patients undergoing surgery: a meta-analysis of randomized controlled trials
Abstract
Background: In anesthetized patients undergoing surgery, the role of lung-protective ventilation with lower tidal volumes is unclear. We performed a meta-analysis of randomized controlled trials (RCTs) to evaluate the effect of this ventilation strategy on postoperative outcomes.
Methods: We searched electronic databases from inception through September 2014. We included RCTs that compared protective ventilation with lower tidal volumes and conventional ventilation with higher tidal volumes in anesthetized adults undergoing surgery. We pooled outcomes using a random-effects model. The primary outcome measures were lung injury and pulmonary infection.
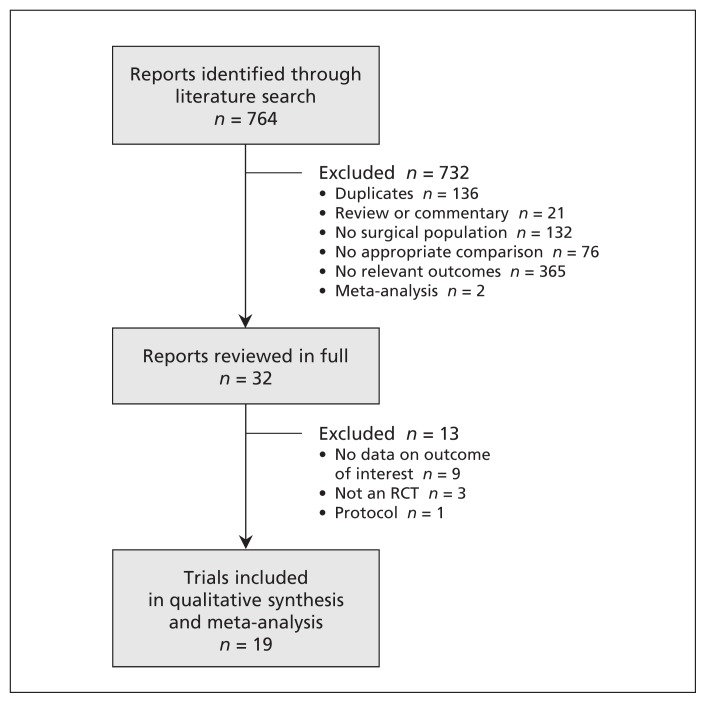
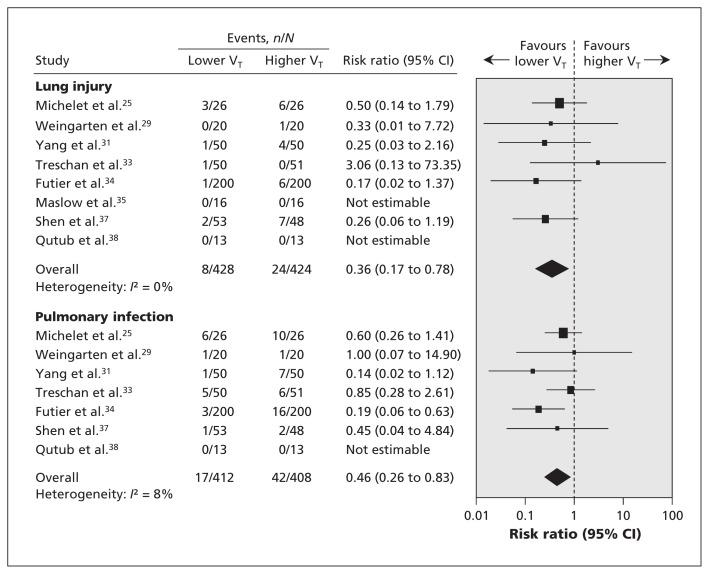
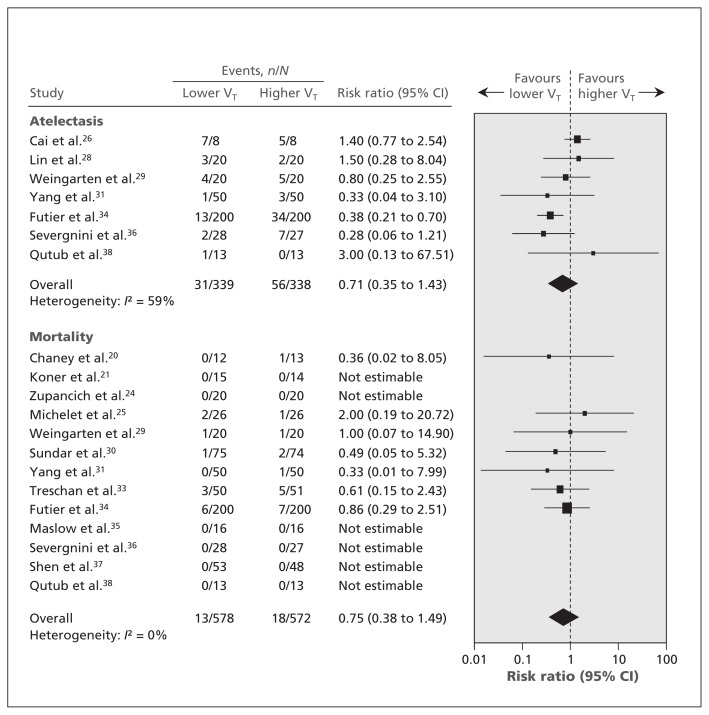
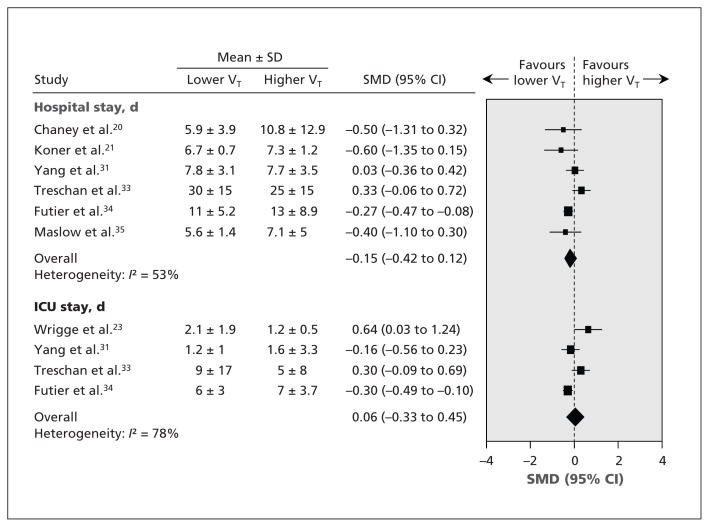
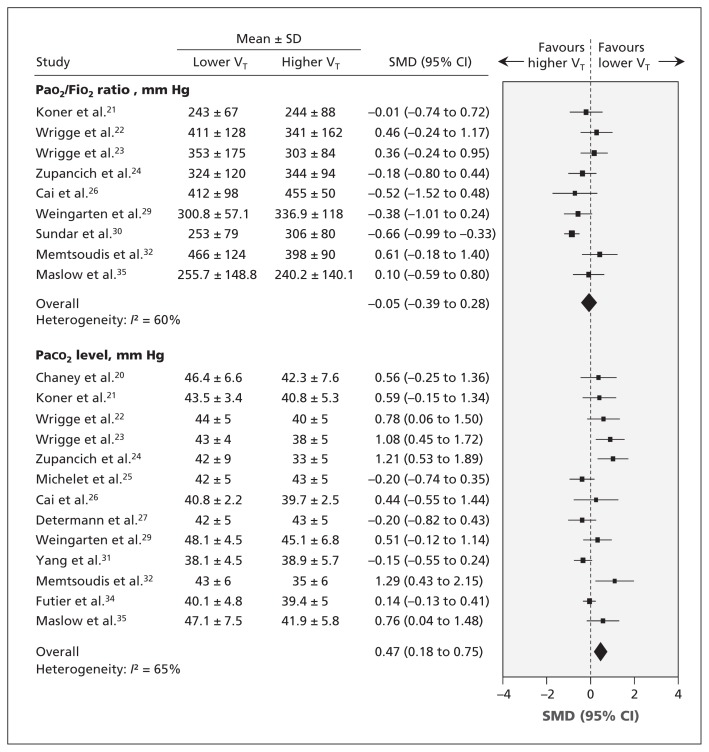
Results: We included 19 trials (n=1348). Compared with patients in the control group, those who received lung-protective ventilation had a decreased risk of lung injury (risk ratio [RR] 0.36, 95% confidence interval [CI] 0.17 to 0.78; I2=0%) and pulmonary infection (RR 0.46, 95% CI 0.26 to 0.83; I2=8%), and higher levels of arterial partial pressure of carbon dioxide (standardized mean difference 0.47, 95% CI 0.18 to 0.75; I2=65%). No significant differences were observed between the patient groups in atelectasis, mortality, length of hospital stay, length of stay in the intensive care unit or the ratio of arterial partial pressure of oxygen to fraction of inspired oxygen.
Interpretation: Anesthetized patients who received ventilation with lower tidal volumes during surgery had a lower risk of lung injury and pulmonary infection than those given conventional ventilation with higher tidal volumes. Implementation of a lung-protective ventilation strategy with lower tidal volumes may lower the incidence of these outcomes.
© 2015 Canadian Medical Association or its licensors.
Figures
References
-
- Weiser TG, Regenbogen SE, Thompson KD, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 2008;372:139–44. - PubMed
-
- Rock P, Rich PB. Postoperative pulmonary complications. Curr Opin Anaesthesiol 2003;16:123–31. - PubMed
-
- Smetana GW, Lawrence VA, Cornell JEAmerican College of Physicians. Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006;144:581–95. - PubMed
-
- Johnson RG, Arozullah AM, Neumayer L, et al. Multivariable predictors of postoperative respiratory failure after general and vascular surgery: results from the Patient Safety in Surgery Study. J Am Coll Surg 2007;204:1188–98. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical